If a doctor just told you you have neovascular glaucoma, the fastest way to protect your vision is to control the underlying retinal disease and lower the eye pressure right away typically with antiVEGF injections+laser, plus pressurelowering meds or surgery. Jumping on these steps early can keep the damage from spiraling out of control.
Both the drugs and the surgeries have clear benefits and real risks, so knowing whats on the table, how the disease progresses, and what realistic outcomes look like helps you and your eyedoctor make the best decisions together.
Understanding the Disease
What is neovascular glaucoma?
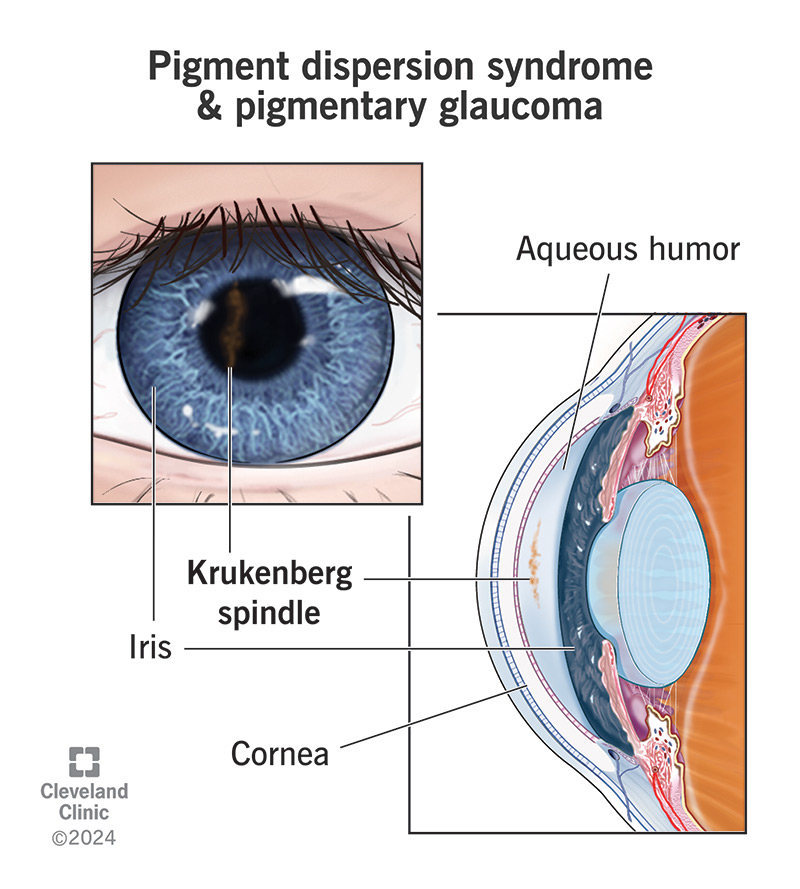
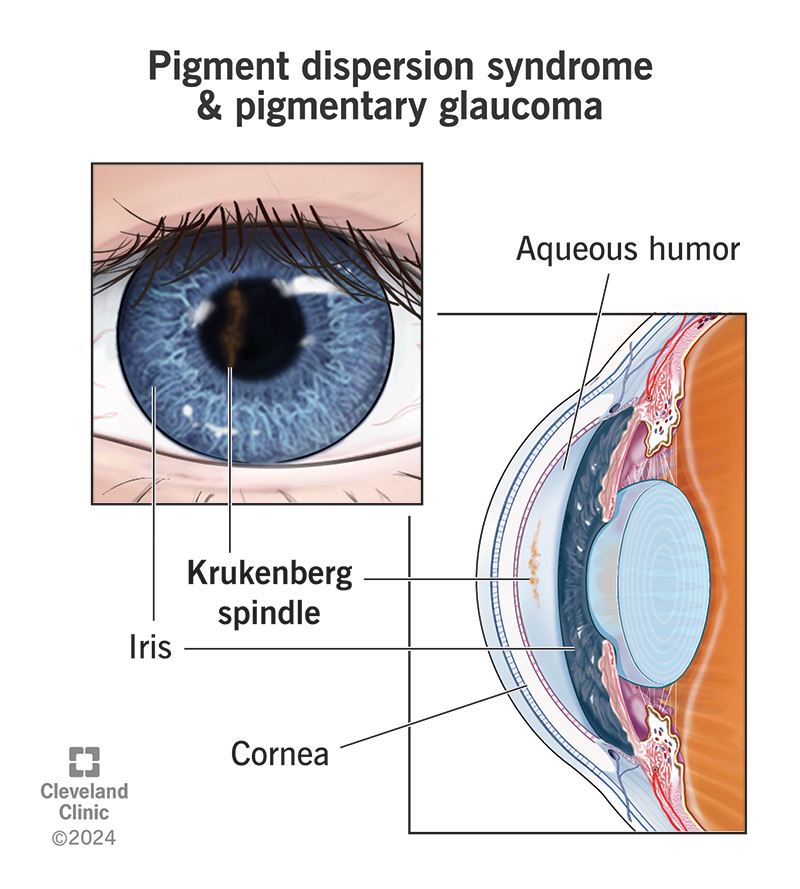
Neovascular glaucoma (NVG) is a type of secondary glaucoma where new, fragile blood vessels grow on the iris and the drainage angle of the eye. These vessels are a response to severe retinal ischemia basically, the back of the eye isnt getting enough oxygen, so it sends out help signals that backfire.
Common causes & risk factors
Think of NVG as the storm warning of eye disease. It usually follows conditions that choke off retinal blood flow, such as:
- Advanced diabetic retinopathy
- Central or branch retinal vein occlusion
- Ocular ischemic syndrome
- Extreme myopia or intraocular tumors (rare)
When any of these , the eye releases vascular endothelial growth factor (VEGF), sparking the unwanted neovascular growth.
How the disease progresses the three stages
NVG doesnt appear fully formed. It evolves through three recognizable phases:
- Preangiogenic stage: Retinal ischemia is present, but new vessels havent formed yet. IOP is still normal.
- Angiogenic stage: New vessels appear on the iris (rubeosis iridis) and start to encroach on the trabecular meshwork.
- Fibrovascular stage: The vessels become scarred, pulling the angle closed and raising intraocular pressure dramatically.
Understanding which stage youre in guides the treatment mix early stages may respond to medication alone, while later stages often need surgery.
Typical symptoms youll notice
NVG can be sneaky. Some people hear the warning signs, others discover it during a routine eye exam. Common clues include:
- Sudden or gradual blurry vision
- Redness or pain in the eye
- Halos around lights
- Headaches that worsen with eye movement
- Visible red patches on the iris (rubeosis)
If any of these appear, especially in the setting of diabetes or a recent retinal vein occlusion, call your ophthalmologist right away.
Treating the Retina
The first weapon against NVG is to stop the VEGFdriven storm at its source.
AntiVEGF drug injections
AntiVEGF drugs such as bevacizumab, ranibizumab, and aflibercept act like a dam, blocking the signal that makes new vessels grow. A typical regimen is one injection every 46 weeks until the neovascular activity calms down.
Benefits:
- Rapid reduction of neovascularization (often within days)
- Minimally invasive just a tiny needle in the side of the eye
- Can be combined safely with laser therapy
Drawbacks:
- Requires repeated visits and injections
- Cost can add up, especially without insurance coverage
- Rare risk of inflammation or infection
Panretinal photocoagulation (PRP) laser
PRP is the firebreak technique for ischemic retina. By burning scattered spots of the peripheral retina, the eyes oxygen demand drops, which in turn reduces VEGF production.
Typical schedule: 1,2002,000 laser burns spread over one or two sessions. The procedure is done in the office, and patients usually feel a brief, uncomfortable flashing sensation.
Pros:
- Longlasting control of VEGF production
- Often eliminates the need for further injections after the initial phase
Cons:
- Can cause peripheral visual field loss (a tradeoff many patients accept)
- May be uncomfortable, especially for those with cataracts
Realworld example
Mark, a 58yearold with proliferative diabetic retinopathy, received three monthly bevacizumab injections followed by a single PRP session. Within two weeks his intraocular pressure (IOP) dropped from 38mmHg to 22mmHg, and the red patches on his iris faded. He now sees clearly enough to read his favorite books again.
Managing Eye Pressure
Even after the retinal storm is calmed, the drainage angle may stay clogged, keeping the pressure high. Thats why we need a second line of defense.
Medical IOPlowering options
Firstline eyedrops include:
- Betablockers (e.g., timolol) reduce fluid production.
- Prostaglandin analogues (e.g., latanoprost) increase outflow.
- Carbonic anhydrase inhibitors (e.g., dorzolamide) lower fluid production.
- Corticosteroid drops control inflammation that can worsen pressure spikes.
According to the , a combination of two or three classes often achieves target IOP (<21mmHg) in the early to mid stages.
When medicines arent enough surgical routes
| Procedure | How It Works | When Its Used | Typical Success Rate | Key Risks |
|---|---|---|---|---|
| Tube shunt (valve) surgery | Implants a tiny tube to drain fluid to an external plate | Advanced fibrovascular stage, uncontrolled IOP despite meds | 7085% achieve IOP 18mmHg | Tube erosion, infection, hypotony |
| Cyclophotocoagulation (CPC) | Laser destroys part of the ciliary body to reduce fluid production | Patients who cant tolerate shunts or have poor visual potential | 6075% lower IOP by 30% | Inflammation, transient vision loss |
| Trabeculectomy (often combined with PRP) | Creates a new drainage pathway under a flap | Selective cases, usually with good visual potential | 5570% maintain target IOP longterm | Bleb failure, infection, scarring |
Choosing the right approach feels a bit like picking a car: you look at your budget, how far you need to go, and what youre comfortable handling. Your surgeon will weigh your disease stage, overall health, and personal preferences before recommending a plan.
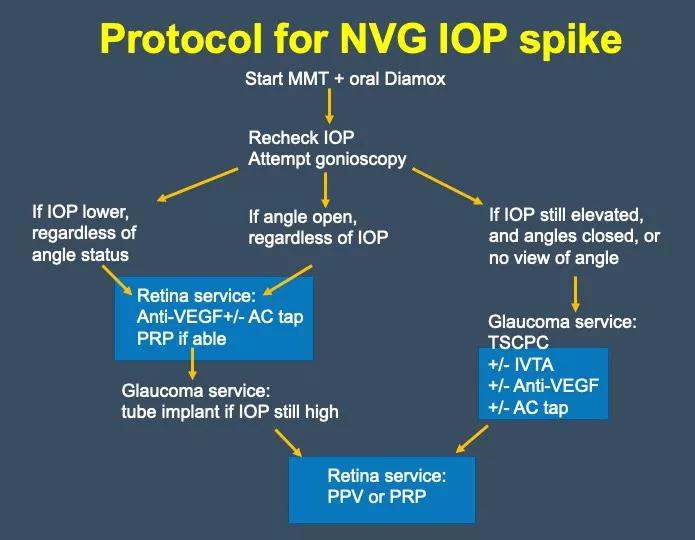
Decisiontree for pressure control
Step1: Start with topical meds + antiVEGF/PRP.
Step2: If IOP stays above 24mmHg after 46 weeks, add a second or third medication class.
Step3: Persistent high pressure discuss tube shunt or CPC.
Step4: In rare cases where the eye is still at risk, a combined trabeculectomy + PRP may be considered.
Can It Be Cured?
The word cure can sound scary, especially when we talk about something as delicate as the eye. In NVG, cure usually means two things:
- Stopping new vessel growth permanently.
- Keeping IOP in a safe range without ongoing surgery.
Modern therapy can stabilize the condition for years, but most experts agree that lifelong monitoring is essential. A 2023 longitudinal study () found that 78% of eyes treated with antiVEGF+PRP maintained vision of 20/40 or better after five years, but only 12% achieved complete cure status (no need for any further treatment).
So, the realistic expectation is control, not eradication. By staying on top of followup appointments and adhering to the treatment plan, you can protect the majority of your sight.
Practical Tools & Resources
Symptom checklist you can print
Keep a small notebook by your bedside and tick off any changes:
- New halos around lights?
- Increasing eye pain or redness?
- Sudden blurry vision?
- Visible red spots on the iris?
If you mark yes to any of these, call your doctor within 24hours.
Printable treatment timeline (PDF)
Having a visual roadmap helps you know when to expect injections, laser sessions, and possible surgery. You can download a free onepage PDF from most major eyecare centers just ask your clinic for a copy.
ICD10 coding guide
When your medical record is updated, clinicians use the ICD10 code H40.5310 for Neovascular glaucoma, unspecified eye. Knowing this code can be handy when youre reviewing insurance statements or discussing your case with a second opinion specialist.
Patientfocused PowerPoint (PPT)
Some hospitals offer a short PPT deck that walks you through the twostep treatment approach antiVEGF+laser, followed by pressurelowering strategies. Its handy for family members who want a quick visual summary.
Balancing Benefits & Risks Making an Informed Decision
Benefit summary
- Preserves central vision in >70% of cases when started early.
- Rapid pressure reduction prevents optic nerve damage.
- Minimally invasive antiVEGF injections have a short recovery time.
- Laser therapy offers lasting control of VEGF production.
Risk & sideeffect overview
- Injectionrelated inflammation (5% of patients).
- Laserinduced peripheral visual field loss (10%).
- Surgical complications: tube erosion, infection, hypotony.
- Medication side effects: dry eye, allergic reactions, systemic betablocker effects for heartsensitive patients.
How to discuss options with your ophthalmologist
Bring a notebook and ask clear, focused questions:
- What stage of neovascular glaucoma am I in?
- If we start antiVEGF now, how many injections will I likely need?
- Should I consider a tube shunt now, or wait to see how the pressure responds?
- What signs mean I should call you immediately?
Having these answers on hand turns a daunting appointment into a collaborative planning session.
Conclusion
Neovascular glaucoma is a fastmoving eye disease, but the good news is that a clear, twostep plantreat the retinal cause with antiVEGF+laser, then bring the eye pressure down with meds or surgerygives most patients a real chance to keep their sight. Understanding the stages, the drug options, and the surgical choices lets you weigh benefits against risks and have a solid conversation with your eye doctor. If youve just received an NVG diagnosis, start the dialogue now, get the recommended injections, and ask about the most suitable pressurelowering strategy for your situation. Your vision is worth that proactive care.
FAQs
What is the first step in treating neovascular glaucoma?
The initial focus is on controlling the underlying retinal ischemia, usually with anti‑VEGF injections combined with pan‑retinal photocoagulation (PRP) laser.
How many anti‑VEGF injections are typically needed?
Most patients receive one injection every 4‑6 weeks until neovascular activity subsides, often requiring 3‑4 monthly doses before switching to PRP alone.
When is a tube shunt surgery considered?
Tube shunt (valve) surgery is recommended for eyes in the fibrovascular stage where intra‑ocular pressure remains >24 mm Hg despite maximal medical therapy and laser treatment.
Can laser photocoagulation cause vision loss?
PRP can lead to peripheral visual field loss in about 10 % of patients, but the trade‑off is long‑term reduction of VEGF production and stabilization of the disease.
What symptoms should prompt an emergency eye‑doctor visit?
New halos around lights, sudden worsening of blurry vision, eye pain or redness, and visible red patches on the iris (rubeosis) require immediate evaluation.