Below youll find the most current recommendations (2024/2023 PDFs), why they matter, and what you should watch out for, so you can feel a little less lost and a lot more empowered.
Why IDSA Guidelines Matter
The Infectious Diseases Society of America (IDSA) is the goldstandard source for managing serious infections. Their panels consist of boardcertified infectiousdisease physicians, microbiologists, and epidemiologists who comb through every relevant study, weigh the quality of evidence, and create consensus recommendations that are peerreviewed before publication.
Because meningitis can turn deadly within hours, clinicians need guidance thats both rapid and reliable. The IDSA guidelines are updated on a regular cycle to incorporate new antibiotics, emerging resistance patterns, and fresh clinical trial data. The most recent releases are the idsa meningitis guidelines 2021 pdf, the idsa meningitis guidelines 2023 pdf, and the justreleased idsa meningitis guidelines 2024. Each version builds on the last, correcting outdated dosing, adding newer adjunctive therapies, and clarifying pediatric nuances.
Core Bacterial Recommendations
When bacterial meningitis pops up on a lab report, every minute counts. The IDSA recommends a standardized empiric regimen that covers the most likely culprits while awaiting culture results. Below is a quick reference table you can print and hand to a clinician.
| Patient Group | Empiric Antibiotics | Typical Dose | Key Notes |
|---|---|---|---|
| Adults18y | Ceftriaxone+Vancomycin | Ceftriaxone 2g IV q12h; Vancomycin 1520mg/kg IV q812h (target trough 1520g/mL) | Add Ampicillin (2g IV q4h) if >50y or immunocompromised (covers Listeria) |
| Children<18y | Cefotaxime+Vancomycin | Cefotaxime 200mg/kg/day IV divided q6h; Vancomycin 15mg/kg IV q6h | For neonates, use Ampicillin+Gentamicin instead |
Adjunctive dexamethasone is another cornerstone. The IDSA advises giving dexamethasone 0.15mg/kg (max 10mg) IV every 6hours, started before or with the first dose of antibiotics. This timing is crucial; giving steroids after antibiotics may miss the window where inflammationmediated neurologic damage can be reduced.
But steroids arent a freepass. They can raise blood glucose, increase risk of gastrointestinal bleeding, and may be less beneficial in older adults with certain comorbidities. The guidelines stress balancing these pros and cons for each patient a classic example of benefits vs. risks that well revisit later.
Viral Meningitis Guidance
Not all meningitis is bacterial. Viral meningitis (often caused by enteroviruses, HSV1/2, or even West Nile virus) typically follows a milder clinical course, but distinguishing it from bacterial disease early on can prevent unnecessary antibiotics.
Typical CSF findings in viral meningitis are:
- Whitecell count: 10300cells/L, predominantly lymphocytes
- Glucose: Normal (45mg/dL)
- Protein: Mildly elevated (100mg/dL)
When a viral cause is suspected, the IDSAs idsa viral meningitis guidelines suggest supportive care: hydration, analgesia for headache, and antipyretics. Antivirals are only recommended for specific pathogens. For example, HSV meningitis warrants IV acyclovir 10mg/kg every 8hours for 1421days. In the vast majority of enteroviral cases, no specific drug is needed, and patients recover within a week.
Pediatric Treatment Insights
Children arent just small adults their immune systems, metabolism, and the organisms that cause meningitis differ. The IDSAs pediatric meningitis guidelines provide agespecific dosing and highlight a few pediatriconly considerations.
| Age | Firstline Antibiotic(s) | Dosage | Duration |
|---|---|---|---|
| Neonates (028days) | Ampicillin+Gentamicin+Thirdgen cephalosporin | Ampicillin 200mg/kg/day IV q12h; Gentamicin 5mg/kg/day IV q24h; Cefotaxime 150mg/kg/day IV q8h | 1021days depending on pathogen |
| Infants (123months) | Ceftriaxone+Vancomycin | Ceftriaxone 100mg/kg IV q12h; Vancomycin 15mg/kg IV q6h | 1014days |
| Children >2years | Ceftriaxone+Vancomycin | Same as adults, weightbased | 1014days |
One hot topic is steroid use in kids. The 2024 IDSA update states dexamethasone may improve hearing outcomes in children with Streptococcus pneumoniae meningitis, but the evidence is less robust than in adults. If a child is under 2years and the pathogen is unknown, many clinicians hold off on steroids until bacterial culture results guide therapy.
Downloading the PDFs
Getting the official documents is easier than you might think. Heres a twostep cheat sheet:
- Go to the IDSAs official (the link opens a new tab).
- Select the year you need 2021, 2023, or 2024 and click Download PDF. The files are typically under 2MB, so they load fast even on a mobile connection.
Whats new in the 2024 version? A short list:
- Revised cefepime dosing for patients with renal impairment.
- New guidance on using linezolid for multidrugresistant Gramnegative organisms.
- Clarified dexamethasone timing now explicitly administer 15minutes before the first antibiotic dose.
Balancing Benefits & Risks
Every medical decision is a scale. Below is a quickchecklist you can run through with your doctor to make sure nothing falls through the cracks.
| Decision Point | Benefit | Potential Risk | How to Mitigate |
|---|---|---|---|
| Start empiric ceftriaxone+vancomycin | Broad coverage against S. pneumoniae, N. meningitidis, and resistant strains | Nephrotoxicity (vancomycin), allergic reactions | Check renal labs, review allergy history, adjust dose if needed |
| Give dexamethasone | Reduces hearing loss and neurologic sequelae | Hyperglycemia, GI bleed | Monitor glucose, consider prophylactic PPI for highrisk patients |
| Use ampicillin for Listeria coverage | Prevents fatal Listeria meningitis in >50y or immunocompromised | Rash, potential for renal toxicity with high doses | Observe for allergic signs, hydrate well |
Realworld example: Sarah, a 34yearold teacher, presented with fever, nuchal rigidity, and a petechial rash. Her ER doctor started the standard ceftriaxonevancomycin combo, added ampicillin because she was 58, and gave dexamethasone within 10minutes of the first antibiotic. Cultures later identified Neisseria meningitidis. Sarah made a full recovery, with no hearing loss exactly what the guidelines aimed for.
Authoritativeness & Trust
To feel confident that youre following the best advice, consider these verification steps:
- Cite the source. The primary reference is the Practice Guidelines for the Management of Bacterial Meningitis (IDSA, 2024). If youre ever unsure, pull up the PDF and check the Recommendations section the wording is identical to what youll hear from your clinician.
- Crosscheck with local protocols. Some hospitals have antimicrobialsteering committees that adapt the IDSA recommendations to regional resistance patterns. Ask your pharmacy or infectioncontrol team for the institutionspecific algorithm.
- Look for peerreviewed backing. Studies such as the NEJM 2022 trial on dexamethasone timing, and the Lancet Infectious Diseases 2023 metaanalysis on cefepime dosing, reinforce the IDSAs conclusions. When you see a recommendation, you can be sure it isnt just opinion.
Remember, the IDSA guidelines are meant to be a tool not a law. Your provider will tailor therapy to your unique situation, taking into account allergies, kidney function, and the exact pathogen once its identified.
Conclusion
Here are the three takeaways you can act on right now:
- Download the latest idsa meningitis guidelines 2024 PDF and keep a printed copy of the empiric antibiotic table handy.
- Make sure dexamethasone (if indicated) is started before or with the first dose of antibiotics timing matters.
- Use the checklist above to discuss benefits and risks with your doctor, and dont hesitate to ask about local resistance patterns or pediatric nuances if a child is involved.
Staying informed empowers you and your loved ones to navigate a frightening diagnosis with confidence. If you have questions, or if youve walked this path before and want to share what helped you, feel free to reach out. Knowledge is the best medicine especially when it comes from trusted, evidencebased sources.
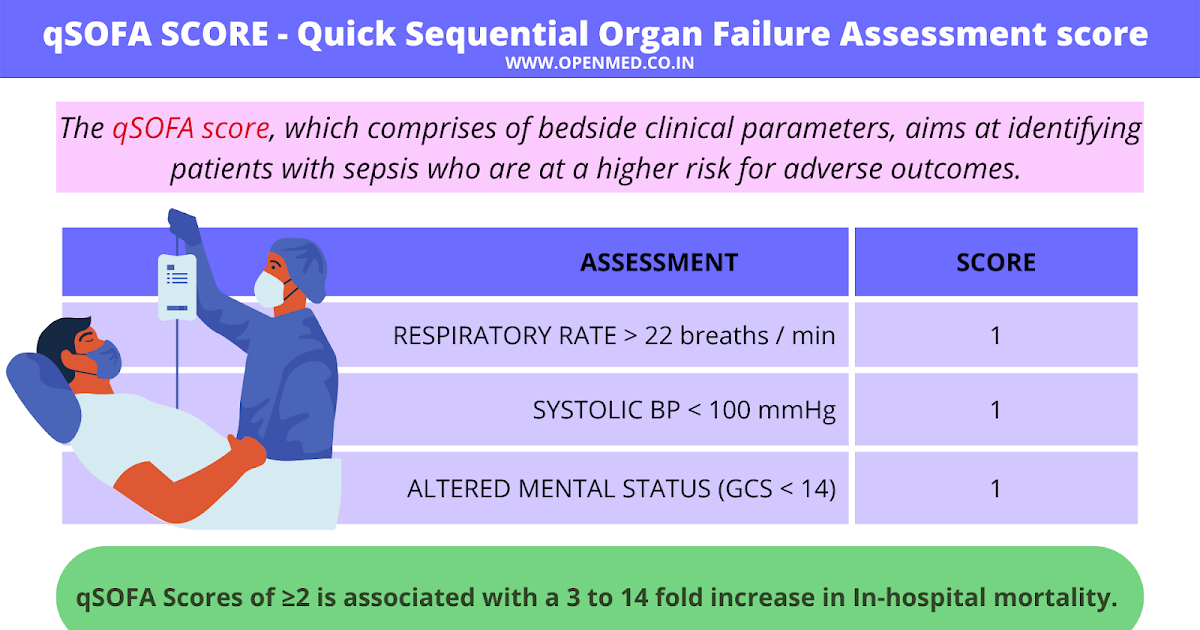
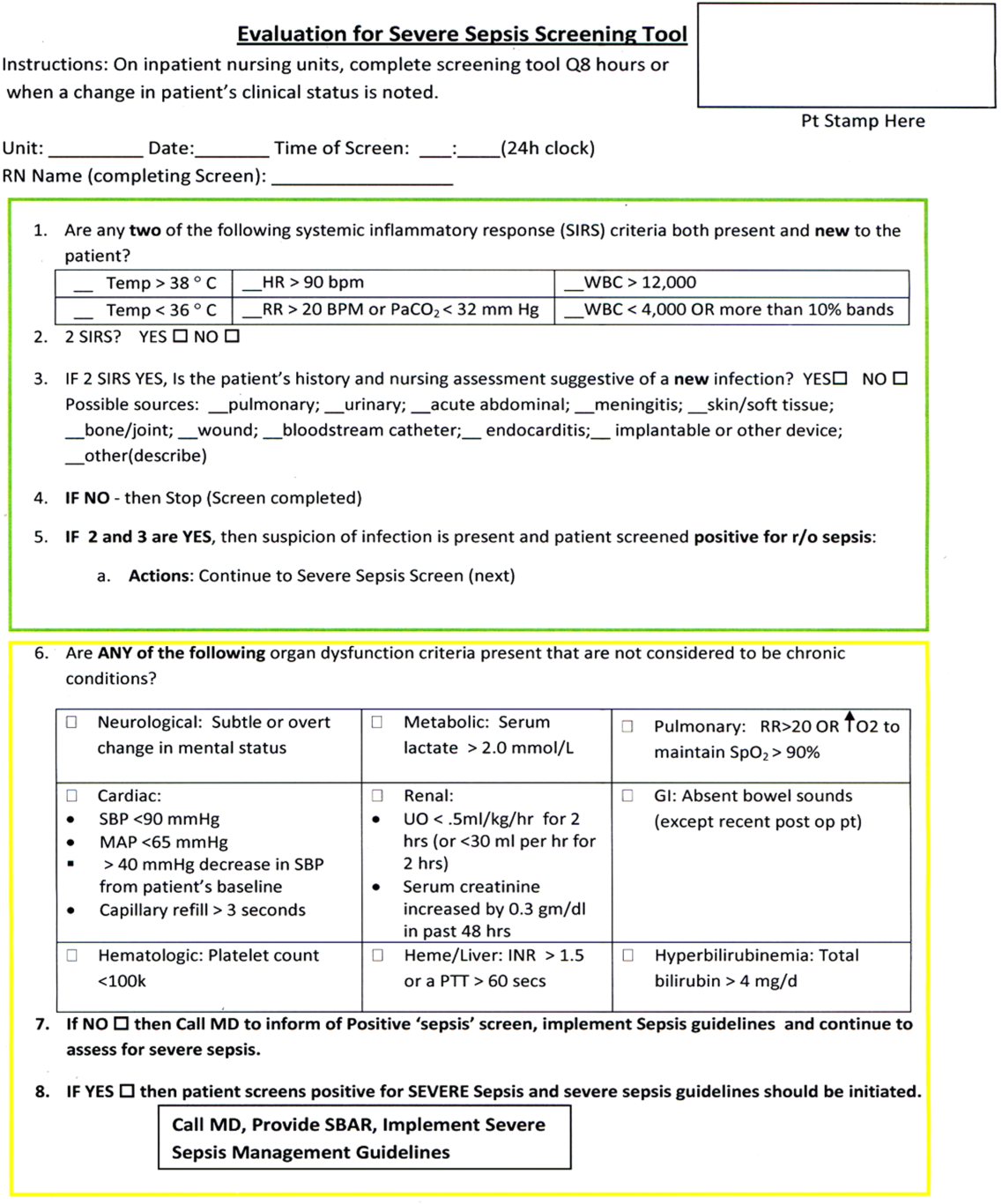
For clinicians and students wanting a quick refresher on assessing organ dysfunction in severely ill patients, consider reviewing tools like the SOFA score, which the critical care community uses to quantify sepsis severity and guide early management decisions.
FAQs
What are the first-line antibiotics recommended by IDSA for bacterial meningitis in adults?
IDSA recommends ceftriaxone combined with vancomycin as empiric therapy for adults, with the addition of ampicillin for patients over 50 or immunocompromised to cover Listeria monocytogenes.
When should dexamethasone be administered according to the IDSA meningitis guidelines?
Dexamethasone should be given 0.15 mg/kg IV every 6 hours, started before or simultaneously with the first dose of antibiotics to reduce inflammation and neurologic damage.
How does the IDSA differentiate treatment approaches between bacterial and viral meningitis?
For bacterial meningitis, prompt empiric antibiotic therapy plus possible adjunctive steroids are advised, while viral meningitis typically requires supportive care, with antivirals only indicated for specific viruses like HSV.
What are the special considerations for treating meningitis in neonates according to IDSA?
Neonates are treated with ampicillin, gentamicin, and a third-generation cephalosporin, with antibiotic dosing and duration tailored by pathogen; steroid use is less well established in this group.
What updates did the 2024 IDSA meningitis guidelines introduce?
The 2024 update includes revised cefepime dosing for renal impairment, guidance on linezolid for multidrug-resistant Gram-negative bacteria, and clarified timing to administer dexamethasone 15 minutes before antibiotics.