Quick answer: Mild Cognitive Impairment (MCI) is a subtle, often reversible slowdown in thinking that usually doesn't stop you from taking care of daily chores, while dementia is a progressive loss of multiple mental abilities that eventually needs support. Knowing which one you're dealing with can shape the care you get, the treatment options you explore, and the peace of mind you deserve.
Let's walk through what each condition looks like, how fast MCI can turn into something more serious, and what you can actually do right now to protect your brain. Grab a cup of tea, settle in, and let's chat about this together.
What Is MCI
Definition & Core Features
MCI sits in that gray zone between normal age-related forgetfulness and full-blown dementia. It's officially described as a measurable decline in one or more cognitive domainsmost often memorywhile everyday activities remain mostly intact. Researchers emphasize that people with MCI can still live independently, but they're on a watchlist for possible progression.
Common Symptoms
Typical signs include:
- Forgetting recent conversations or appointments but remembering long-term memories.
- Struggling to find the right word during a chat.
- Needing a little extra time to process information (like a slower mental WiFi).
- Occasional difficulty planning or organizing simple tasks.
Imagine a friend who always knows the route home but suddenly forgets where they left their glasses. That's MCI in a nutshellannoying, but not yet disabling.
Who Gets MCI?
Most studies show the average age for mild cognitive impairment falls between 60 and 80 years. Roughly 1 in 10 people over 65 meet criteria for MCI at any given time.
Causes & Risk Factors
There isn't a single culprit; rather, a mix of factors can tilt the brain toward MCI:
- Vascular issues such as hypertension or diabetes.
- Sleep disorders (especially sleep apnea).
- Depression or chronic stress.
- Certain medications that affect cognition.
- Genetic predispositions, like the APOE4 allele.
When you hear "risk factor," think of it as a warning signsomething you can often modify with lifestyle tweaks or medical care.
What Is Dementia
Definition & Diagnostic Criteria
Dementia is a syndrome that involves a significant decline in at least two cognitive domains (memory, language, executive function, visual-spatial skills, or personality), severe enough to interfere with daily living. The DSM-5 outlines these criteria, and clinicians typically confirm the diagnosis with a battery of neuropsychological tests and brain imaging.
Main Types
While dementia is the umbrella term, the most common subtypes are:
- Alzheimer's disease the classic memory-first dementia.
- Vascular dementia caused by reduced blood flow to the brain.
- Lewy-body dementia marked by visual hallucinations and movement problems.
- Frontotemporal dementia early changes in personality and behavior.
Each type has its own pattern of progression, but they all share the core challenge: the brain's ability to function declines over time.
Typical Symptom Progression
Most people experience a fairly predictable trajectory:
- Early stage: Short-term memory loss, occasional word-finding trouble.
- Middle stage: Difficulty with complex tasks, disorientation, mood swings.
- Late stage: Severe memory loss, inability to communicate, full dependence on caregivers.
Visualizing this timeline helps families plan aheadwhether it's arranging home modifications or exploring long-term care options.
Average Age of Onset & Prevalence
Dementia usually appears after age 65, affecting roughly 1 in 9 people over that age. Prevalence rises sharply after 80, underscoring the importance of early detection.
Direct Comparison
| Aspect | MCI | Dementia |
|---|---|---|
| Cognitive domains affected | Usually one (most often memory) | Two or more (memory + language, reasoning, etc.) |
| Impact on daily life | Minimal; independence usually maintained | Significant; assistance often required |
| Progression risk | 1015% per year to dementia | Progressive and irreversible |
| Typical diagnostic tools | MoCA, MMSE, brief neuropsych tests | Comprehensive neuropsych battery + MRI/CT |
| Underlying cause | Varied (vascular, metabolic, medication) | Specific disease process (Alzheimer's, vascular, etc.) |
MCI vs Dementia vs Alzheimer's
It's easy to mix these up because the terms overlap. Alzheimer's is a specific type of dementia, not a separate condition. MCI can be a precursor to Alzheimer's, but many people with MCI never develop any form of dementiaespecially if they adopt brain-healthy habits.
MCI vs Dementia MoCA Scores
The Montreal Cognitive Assessment (MoCA) is a quick 30-point test that clinicians love for its sensitivity. Rough guidelines:
- Score 26 = Normal cognition.
- Score 2325 = MCI.
- Score 22 = Possible dementia.
These cutoffs aren't absolute, but they give doctors a useful snapshot.
How Fast MCI Progresses
Conversion Statistics
Research consistently shows that about 1015% of people with MCI transition to dementia each year. Over a five-year span, the risk climbs to roughly 3050%.
Factors That Accelerate Progression
Not everyone follows the same timeline. Certain red flags increase the odds of a quicker decline:
- Age >75.
- Presence of the APOE4 gene.
- Concurrent vascular disease (high blood pressure, stroke history).
- Low educational attainment or limited mental stimulation.
- Depression or chronic anxiety.
When MCI Stays Stableor Improves
Good news: up to 40% of people with MCI remain stable or even improve, especially when they adopt evidence-based lifestyle changes. Dietary adjustments, stress management techniques, and cognitive training are key contributors to a slower or reversed trajectory.
Real-World Example
Take Jane, 68, who noticed she kept misplacing her keys. After a mild cognitive impairment test, her doctor recommended a Mediterranean diet, regular brisk walks, and a weekly brain-gym class. Two years later, Jane's MoCA score rose from 23 to 27, and she reports feeling sharper than ever.
Diagnosis and Testing
Mild Cognitive Impairment Tests
The most common screening tools are:
- MoCA good for detecting subtle deficits.
- MMSE (Mini-Mental State Examination) widely used, though slightly less sensitive for MCI.
- Clock-Drawing Test quick visual-spatial check.
These tests are brief (often under 15 minutes) and can be administered by a primary-care physician, neuropsychologist, or trained nurse.
Dementia Assessment Toolbox
When dementia is suspected, doctors add:
- A comprehensive neuropsychological battery covering memory, language, executive function, and more.
- Brain imaging (MRI or CT) to look for atrophy patterns, vascular lesions, or other structural changes.
- Blood work to rule out reversible causes (thyroid issues, vitamin B12 deficiency, infections).
Who Should Get Tested?
If you or a loved one experiences:
- Repeated memory lapses that worry you.
- Changes in decision-making or judgment.
- Difficulty completing familiar tasks.
- A family history of Alzheimer's or other dementias.
Don't wait. Early assessment opens doors to treatment, planning, and peace of mind.
Treatment and Management
Can MCI Be Reversed?
There's no magic pill, but science backs several interventions that can slow or even improve MCI symptoms:
- Physical activity aerobic exercise 150 minutes per week boosts brain-derived neurotrophic factor (BDNF), supporting neuronal health.
- Mediterranean diet rich in leafy greens, fish, nuts, and olive oil, it's associated with lower risk of cognitive decline.
- Cognitive training puzzles, learning a new language, or brain-training apps keep neural pathways active.
- Sleep hygiene 79 hours of quality sleep clears amyloid plaques.
- Managing cardiovascular health controlling blood pressure, cholesterol, and diabetes reduces vascular contributions.
- Addressing stress caused headaches and chronic stress, which can negatively impact cognitive function.
These steps are not just nice to have; randomized controlled trials show measurable improvements in MoCA scores for participants who followed a combined lifestyle program.
Dementia Slowing the Progression
When dementia is diagnosed, treatment shifts to maintaining function and quality of life:
- FDA-approved meds such as donepezil, rivastigmine, or memantine can modestly improve cognition and daily functioning.
- Non-pharmacologic strategies music therapy, reminiscence groups, and structured daily routines.
- Support services caregiver education, respite care, and community resources.
Shared Strategies for Both Conditions
Whether you're navigating MCI or dementia, these fundamentals apply:
- Keep blood pressure, glucose, and cholesterol in check.
- Quit smoking and limit alcohol.
- Stay socially engagedregular contact with friends or family buffers stress.
- Address depression early; mood disorders can masquerade as cognitive decline.
How to Reverse Cognitive Decline?
"Reverse" is a strong word, but many people experience meaningful stabilization or improvement when they commit to the above strategies. The key is consistencythink of it like training for a marathon, not a quick sprint.
Real World Perspectives
Patient Story Living with MCI
Mark, 62, first noticed he was forgetting appointments despite keeping a digital calendar. After a mild cognitive impairment test, he was told his brain was still healthy but needs a boost. He joined a local walking group, swapped processed snacks for nuts and berries, and started a weekly crossword puzzle club. Six months later, Mark says, "I actually feel sharper. My wife stopped worrying, and I'm back to enjoying my hobbies."
Caregiver View When MCI Turned into Dementia
Sarah cared for her mother, Ellen, who was diagnosed with MCI at 71. Over three years, Ellen's memory lapses grew worse, and she began needing help with cooking and budgeting. A neurologist confirmed a transition to early-stage Alzheimer's dementia. Sarah's biggest takeaway? "Early detection gave us time to arrange home modifications, join a support group, and plan legal matters. It wasn't easy, but it softened the shock."
Bottom Line Summary
To wrap things up, here are the takeaways you can act on today:
- MCI is a warning sign, not a death sentence. It often stays stable, especially with lifestyle changes.
- Dementia is progressive. Early diagnosis, medical treatment, and support services can preserve quality of life.
- Screening matters. Simple tools like the MoCA can differentiate MCI from dementia quickly.
- Take charge of your brain health. Exercise, a Mediterranean diet, good sleep, and mental challenges are your best allies.
- Don't walk alone. Reach out to healthcare providers, support groups, and trusted friends.
If this resonated with you, why not download our free MCI vs Dementia QuickGuide (link in the sidebar) and share your thoughts below? Have you or someone you love faced this crossroads? Your story might help another reader feel less alone.
FAQs
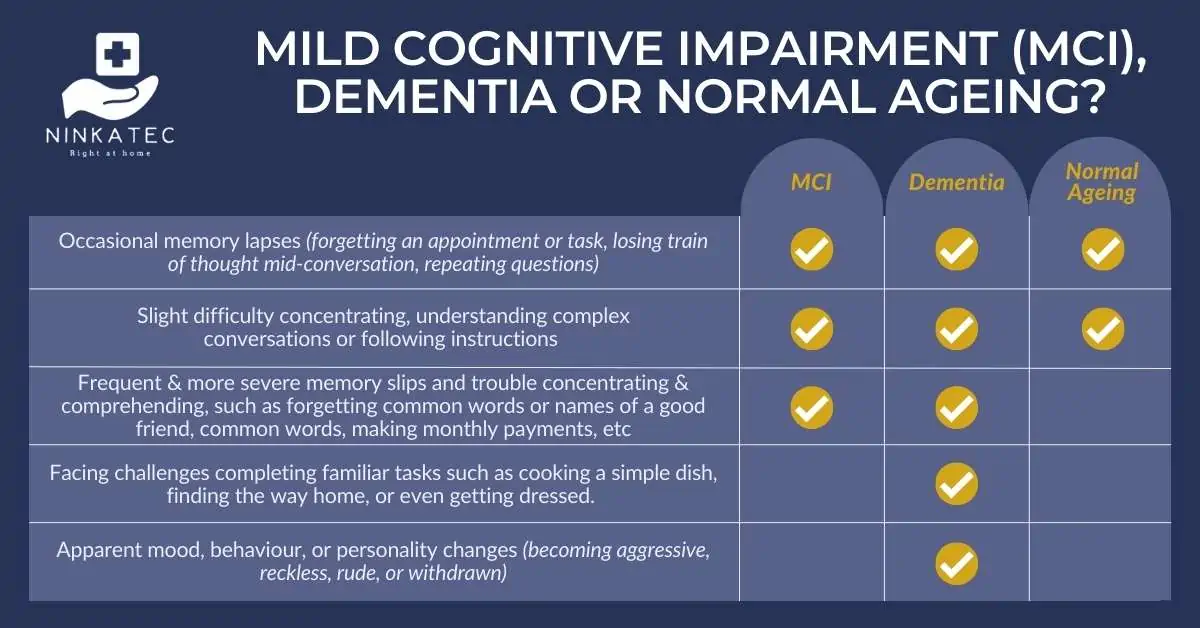
What is the main difference between MCI and dementia?
MCI involves mild, often reversible cognitive decline with preserved daily function, while dementia entails progressive loss of multiple mental abilities that interferes with everyday living.
How likely is it that MCI will progress to dementia?
On average, 10‑15% of people with MCI convert to dementia each year; over five years the risk rises to roughly 30‑50%, though many remain stable or improve.
Can lifestyle changes reverse MCI?
While there’s no cure, regular aerobic exercise, a Mediterranean diet, cognitive training, good sleep, and cardiovascular risk management can stabilize or even improve MCI symptoms.
Which tests are used to diagnose MCI versus dementia?
MCI is usually screened with brief tools like the MoCA, MMSE, or Clock‑Drawing Test. Dementia assessment adds comprehensive neuropsychological batteries, brain imaging, and lab work to rule out reversible causes.
What treatments are available for dementia?
FDA‑approved medications such as donepezil, rivastigmine, and memantine may modestly improve cognition. Non‑pharmacologic strategies—music therapy, structured routines, and caregiver support—focus on quality of life.