Youve just learned you have a pituitary macroadenoma. The good news is that most people find reliefwhether through a medication, a minimallyinvasive surgery, or preciselytargeted radiation. Below youll get straighttothepoint answers about the options that actually work, the risks you should weigh, and what life looks like after treatment.
Lets skip the jargon and dive right in. Imagine were sitting with a cup of coffee, and Im sharing the roadmap that can shrink that tumor, balance your hormones, and get you back to feeling yourself again.
Understanding Macroadenomas
What are the main symptoms?
Typical signs
Macroadenomas are larger than 10mm, so they often make themselves known. Common complaints include:
- Persistent headaches like a dull throb that wont quit.
- Vision changes, especially loss of peripheral (side) vision.
- Hormonal excess (e.g., unexplained weight gain, menstrual irregularities for women, or unexpected growth of facial hair for men).
- Fatigue, mood swings, or difficulty concentrating.
If any of these feel familiar, its worth chatting with a specialist sooner rather than later.
How is it diagnosed?
Imaging and labs
Doctors start with a magnetic resonance imaging (MRI) scanoften called the gold standard for spotting pituitary tumors. A contrastenhanced MRI can show the exact size and whether the tumor is pressing on nearby structures.
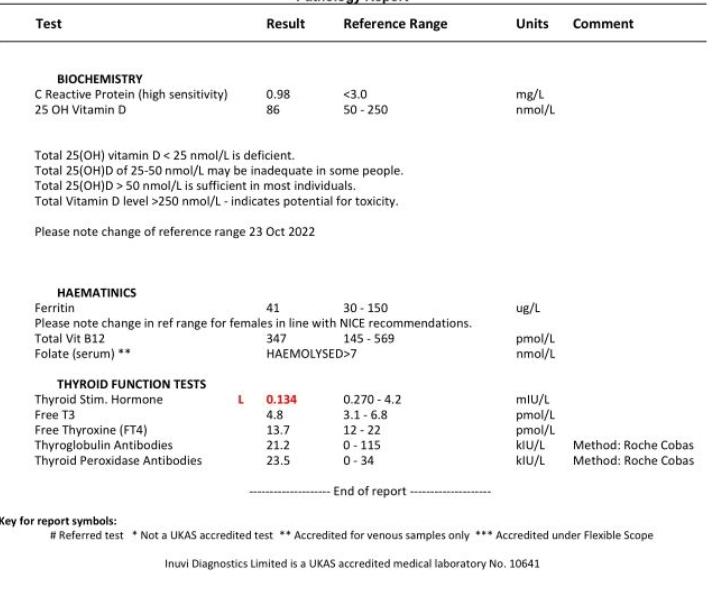
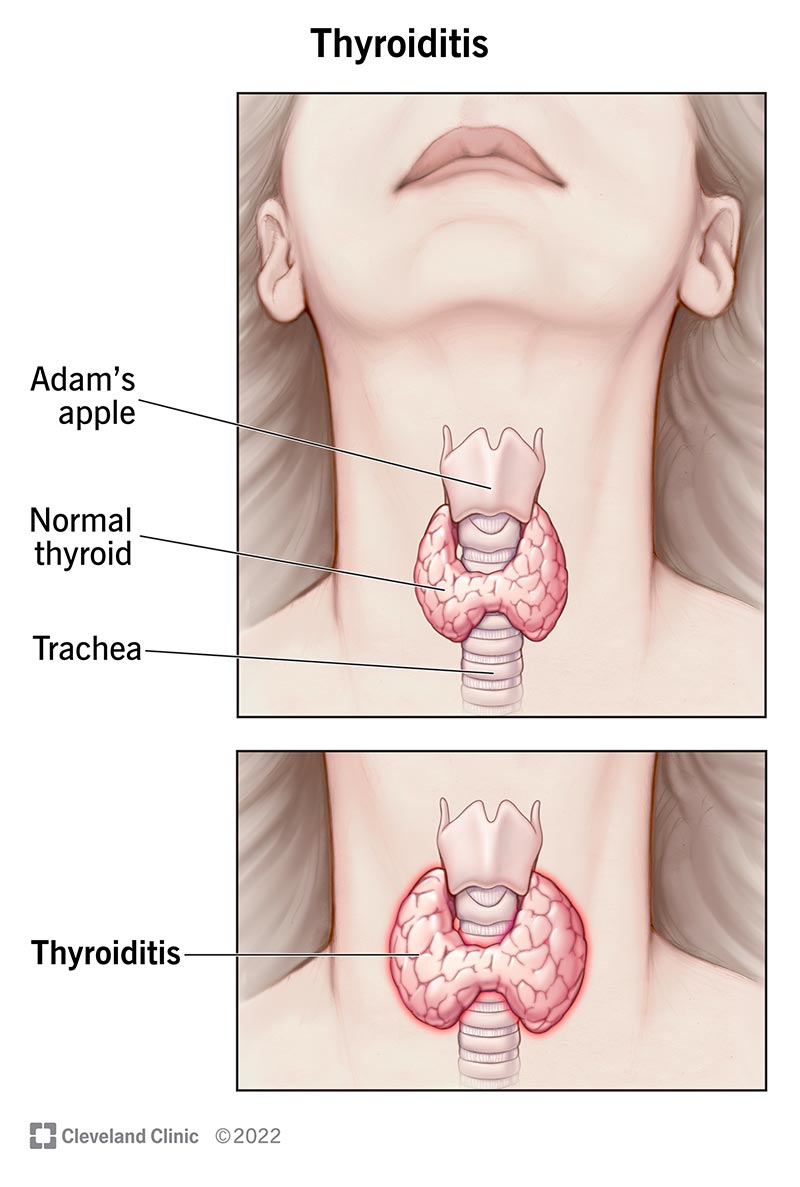
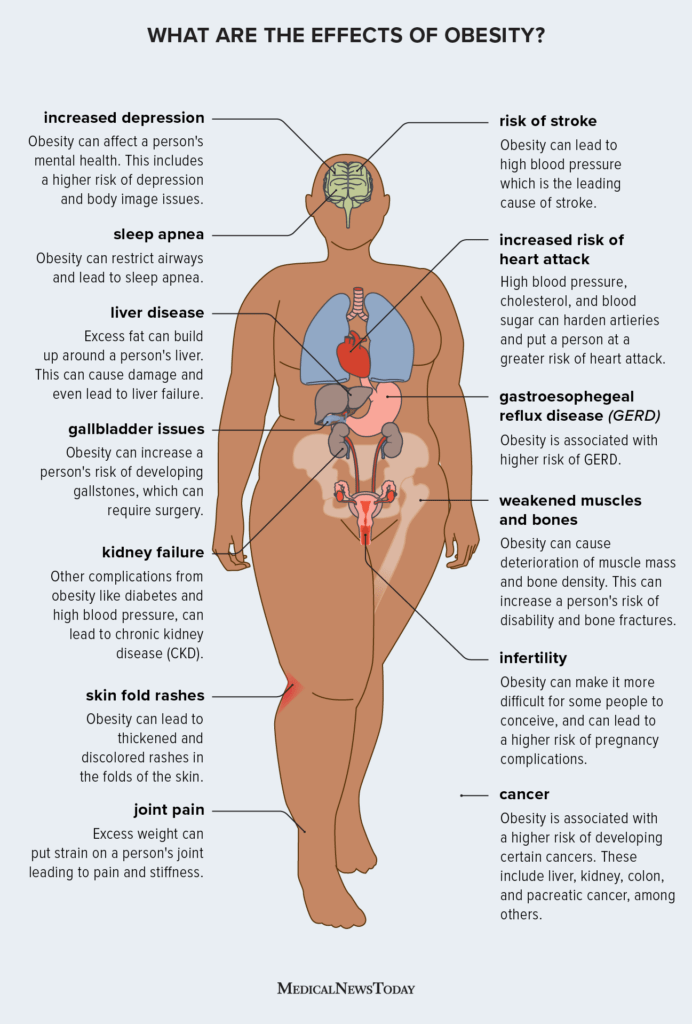
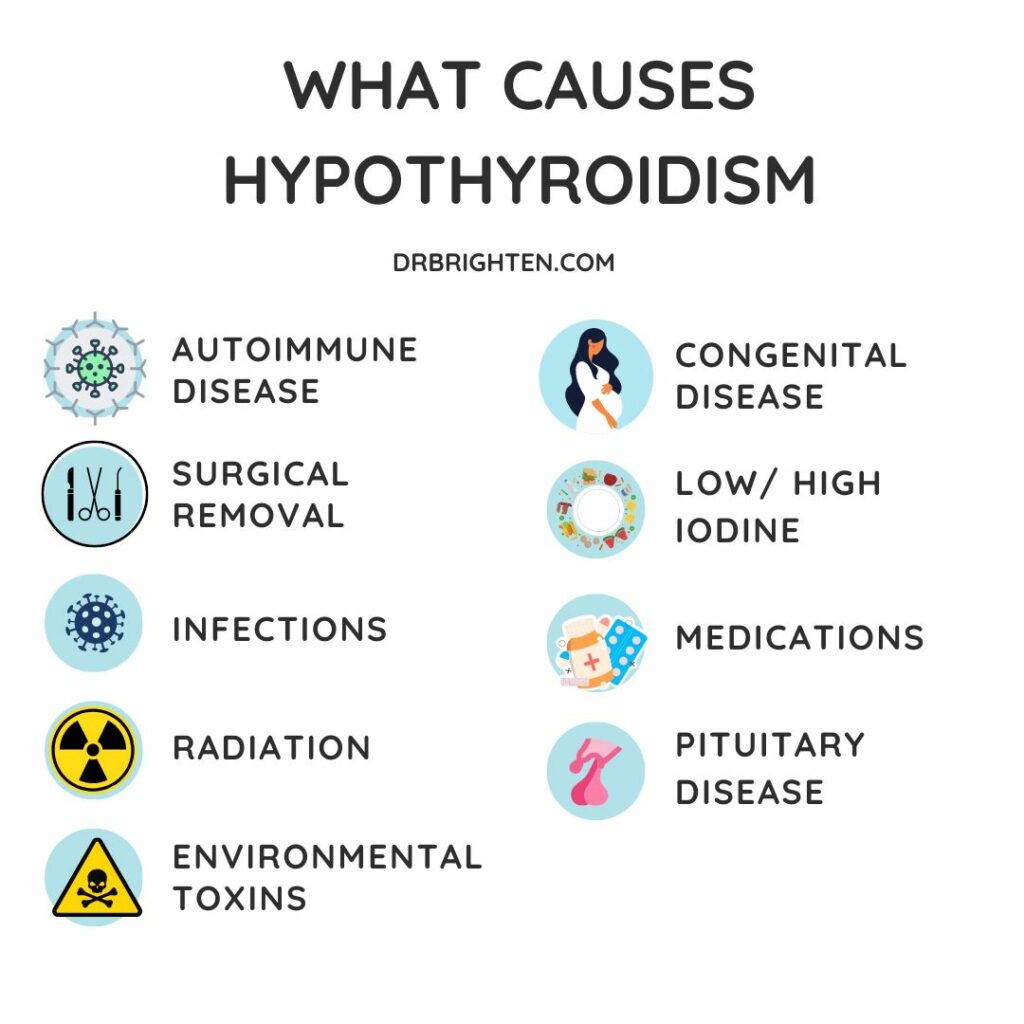
Blood tests for pituitary hormones (prolactin, IGF1, cortisol, TSH, LH/FSH, etc.) help determine if the adenoma is secreting hormones or causing deficiencies. In the case where hormone deficiency is present, it's important to consider related conditions like thyroid hormone deficiency. For hypothyroidism, see more on the key hypothyroidism effects, as these may overlap or be exacerbated by pituitary dysfunction. Essentially, a complete hormonal panel is essential for treatment planning.
Macroadenoma vs. Microadenoma
Key differences
| Feature | Macroadenoma | Microadenoma |
|---|---|---|
| Size | >10mm | 10mm |
| Symptoms | Often visual or masseffect symptoms | Usually silent or mild hormonal changes |
| Firstline treatment | Often surgery or a combination | Medication frequently enough |
Medication Options
Dopamine agonists and beyond
When the tumor secretes prolactin, dopamine agonists like cabergoline or bromocriptine are frontline heroes. They can shrink the tumor by up to 50% in many cases and restore normal prolactin levels.
If the adenoma produces growth hormone, somatostatin analogs (e.g., octreotide, lanreotide) and GH receptor antagonists (pegvisomant) are the goto drugs. These medications help control the hormonal excess and may also reduce tumor size.
How to shrink a pituitary tumor naturally?
Science tells us that no food will cure a macroadenoma, but a balanced diet can support overall hormone health. Aim for a lowglycemic, antiinflammatory eating planthink plenty of leafy greens, fatty fish, nuts, and berries. Regular moderate exercise and adequate sleep help keep cortisol and insulin in check, which indirectly supports pituitary function.
Foods to avoid with a pituitary tumor
Certain foods can aggravate hormonal imbalances:
- Excessive refined sugars and highfructose corn syrup.
- Processed soy products (they contain phytoestrogens that may interfere with hormone pathways).
- Overcaffeinated drinks, which can spike cortisol.
- Heavy alcohol consumption, which disrupts pituitary signaling.
Swap these for wholegrain carbs, fresh fruits, and plenty of water to stay hydrated.
Surgical Solutions
Transsphenoidal surgery
The transsphenoidal approach is the most common technique for macroadenoma removal. A surgeon works through the nose and sphenoid sinus, avoiding a large scalp incision. Modern endoscopic tools give a panoramic view, allowing precise tumor removal while preserving surrounding tissue.
Success rates are higharound 8090% of patients achieve at least 70% tumor reduction, and many experience immediate vision improvement.
Comparison of surgical approaches
| Approach | Invasiveness | Recovery Time | Complication Rate |
|---|---|---|---|
| Endoscopic Endonasal (EEEA) | Minimally invasive | 12days hospital stay; 23weeks to normal activity | ~5% (CSF leak, nasal issues) |
| Traditional Transsphenoidal | Slightly more invasive | 23days hospital stay; 34weeks recovery | ~8% |
| Transcranial | Open skull surgery | 57days hospital stay; 68weeks recovery | ~15% |
When is transcranial surgery needed?
For giant macroadenomas that spill into the cavernous sinus or extend far behind the brain, a transcranial route may be the safest option. It provides direct access, but the tradeoff is a longer recovery and a higher risk of complications such as memory issues or facial nerve changes.
Radiation Therapy
Conventional vs. stereotactic
Radiation is usually considered after surgery if any tumor tissue remains, or when surgery isnt feasible. Conventional fractionated radiation delivers small doses over several weeks, gently eroding the tumor.
Stereotactic radiosurgery (Gamma Knife or CyberKnife) delivers a single highdose beam with pinpoint accuracy. Its ideal for small residual tumors and has a lower risk of damaging surrounding brain tissue.
According to the National Cancer Institute, most patients achieve tumor control within 510years after stereotactic treatment, though lifelong hormone monitoring is essential.
Life After Treatment
Recovery timeline
First 24hours: After endoscopic surgery, youll be in a recovery room with a nasal pack to control bleeding. Most people feel groggy but can sit up within a few hours.
First 24 weeks: Light activity is encouragedshort walks, gentle stretching. Avoid heavy lifting, strenuous cardio, or noseblowing that could disturb the surgical site.
Hormone monitoring and blood tests
Regular blood work is the compass guiding your recovery. Typical labs include:
- Prolactin
- IGF1 (for growthhormone excess)
- Cortisol and ACTH
- TSH and free T4
- LH/FSH (especially for women planning pregnancy)
Doctors usually order these tests every 36months for the first year, then annually if everything stays stable.
Lifestyle guidance
Foods to keep and foods to skip
Reinforce the earlier listlean proteins, omega3 rich fish, and colorful vegetables are your allies. Stay clear of processed sugars, excessive soy, and highcaffeine beverages.
Exercise, sleep, and stress
Regular moderate exercise (30minutes of brisk walking or swimming) improves circulation and supports hormonal balance. Aim for 78hours of sleep, and practice stressrelief techniquesdeep breathing, yoga, or even a favorite hobby.
Life expectancy and quality of life
Most studies show that individuals with treated pituitary adenomas have a normal life expectancy, especially when hormone deficiencies are adequately replaced. In some cases, patients may experience primary hypothyroidism as a result of pituitary damage, making ongoing hormone monitoring and management critical. A 2022 metaanalysis of over 5,000 patients reported a 5year survival rate of 96% after successful surgery.
Women may worry about menstrual changes or fertilitythese are common, but endocrinologists can tailor hormone replacement to restore regular cycles and support pregnancy when desired.
Expert Insights & Trusted Resources
Why expertise matters
Choosing a surgeon who performs at least 30 pituitary surgeries a year dramatically improves outcomes. Look for board certification, a high volume of endoscopic cases, and patient testimonials that mention quick visual recovery.
Recommended reading
- National Cancer Institute Pituitary Cancer Overview
- 2024 Endocrine Society Clinical Practice Guideline on Pituitary Adenomas (available on their website).
How to verify a providers authority
Check the doctors credentials on the American Board of Neurological Surgery or the American Association of Clinical Endocrinologists. High surgical volume, research publications, and membership in professional societies are good signs of authority.
Conclusion
Macroadenoma treatment isnt a onesizefitsall road; medication, minimallyinvasive surgery, and targeted radiation each have clear benefits and risks. Knowing the symptoms, staying on top of hormone labs, and following postop lifestyle tips (including the foods to avoid) empowers you to make informed choices and enjoy a normal life expectancy. If youve just received a diagnosis, reach out to a pituitaryspecialist, ask about the endoscopic endonasal approach, and consider downloading a posttreatment checklist. Your journey starts with the right information, and you deserve a path that feels both safe and hopeful.
FAQs
What are the first‑line treatment options for a macroadenoma?
Most macroadenomas are managed with medication (e.g., dopamine agonists for prolactin‑secreting tumors), endoscopic transsphenoidal surgery, or stereotactic radiation if surgery isn’t feasible.
How effective is transsphenoidal surgery for shrinking macroadenomas?
Endoscopic transsphenoidal surgery achieves 70‑90 % tumor reduction in the majority of patients, often with immediate improvement in vision and headaches.
Can radiation therapy be used as the sole treatment for macroadenomas?
Radiation is typically reserved for residual tumor after surgery or when surgery is contraindicated; it’s rarely used alone because hormonal control is slower.
What hormonal tests are needed after treatment?
Patients need regular labs for prolactin, IGF‑1, cortisol, ACTH, TSH, free T4, and LH/FSH every 3‑6 months initially, then annually if stable.
Are there lifestyle changes that help after macroadenoma treatment?
Yes—maintain a balanced low‑glycemic diet, regular moderate exercise, adequate sleep, and stress‑management techniques to support hormone balance and overall recovery.