Hey there, friend. If youve just found out you or someone you love carries a Lynchsyndrome mutation, the first thought that probably pops up is, What now? The answer is surprisingly simple: follow the right screening routine, and you can stay a step ahead of cancer. Below, Im breaking down the latest lynch syndrome screening guidelines in a friendly, easytoread wayno medical jargon overload, just clear steps you can act on today.
Quick Summary
What are the NCCNbacked guidelines?
The National Comprehensive Cancer Network (NCCN) recommends a tiered surveillance plan that starts earlyoften in your 20s for most gene carriersand intensifies as you age. Think of it as a personalized safety net that catches potential problems before they become serious.
Key Takeaway Table
| Guideline Body | Start Age | Screening Frequency | Primary Test |
|---|---|---|---|
| NCCN (2024) | 2025 (MLH1/MSH2), 30 (MSH6), 35 (PMS2) | Colonoscopy every 12years | Colonoscopy, Upper GI endoscopy |
| USMSTF (2023) | Same as NCCN | Same | Same |
| AGA (2022) | 2530 | Every 2years | Colonoscopy |
Colonoscopy Guidance
How often should colonoscopies be done?
For most Lynchsyndrome carriers, a colonoscopy every 12years is the gold standard. The NCCN says start at age2025 if you have an MLH1 or MSH2 mutation, at 30 for MSH6, and at 35 for PMS2. The idea is to catch precancerous polyps early when theyre easiest to remove.
Why the difference by gene?
MLH1 and MSH2 mutations tend to cause cancers earlier, so the screening kicks in sooner. MSH6 and PMS2 generally have a later onset, which is why the start ages shift a bit later. If youre unsure which gene you carry, a quick chat with your genetics counselor can clear it up.
What makes a good prep?
A clear bowel prep is crucialthink of it like cleaning a window before you paint. Inadequate prep can hide small polyps, and you might end up needing another exam sooner than planned. Ask your gastroenterologist about splitdose prep options; many patients find them easier to tolerate.
Colonoscopic Schedule by Gene
| Gene | Start Age | Interval |
|---|---|---|
| MLH1 | 2025 | Every 12years |
| MSH2 | 2025 | Every 12years |
| MSH6 | 30 | Every 12years |
| PMS2 | 35 | Every 12years |
UpperGI Endoscopy
Why add an upper GI exam?
Historically, we focused on colon health, but research shows that people with Lynch syndrome also have higher risks for stomach and duodenal cancers. A 2020 study published in Gastroenterology highlighted that early detection via upperGI endoscopy can significantly lower mortality rates.
When should it start?
The NCCN suggests beginning upperGI surveillance at age3035, with repeat exams every 35years. If you have a family history of gastric cancer, your doctor might suggest starting a bit earlier.
What to expect?
During the procedure, a thin, flexible tube with a camera slides down your throat. It feels similar to a regular endoscopysome pressure, a bit of discomfort, but usually not painful. Most people are out of the recovery room in under an hour.
Gynecologic & Other Organ Surveillance
Endometrial and ovarian monitoring
Women with Lynch syndrome face a higher risk of endometrial and ovarian cancers. The NCCN recommends an annual endometrial biopsy or a transvaginal ultrasound starting at age3035, and repeating every 12years. While its not a perfect test, it adds a valuable safety layer.
Urinary tract and pancreas
Although the risk is lower, some experts suggest periodic imaging (like MRI or ultrasound) for the urinary tract and pancreas, especially if you have a strong family history of those cancers. Its an optional, yet prudent, addition to your plan.
Genetic Testing & Cost
How is Lynch testing performed?
Most labs use a blood draw or a saliva kitboth are equally accurate. A blood test for Lynch syndrome often costs between $1,500 and $3,000, but many insurance plans cover it fully or partially. If youre uninsured, look for programs that offer reducedprice testing; some national foundations even provide free kits for qualifying families.
Is an athome test reliable?
Yes, reputable companies ship a saliva collection tube that you return by mail. The key is to choose a lab thats CLIAcertified and accredited by the College of American Pathologists. Beware of quickfix services that arent transparent about their methodology.
Where to find cost info?
The offers a costestimator tool that helps you understand outofpocket expenses based on your insurance provider.
Understanding Bethesda Criteria
What are the Bethesda criteria?
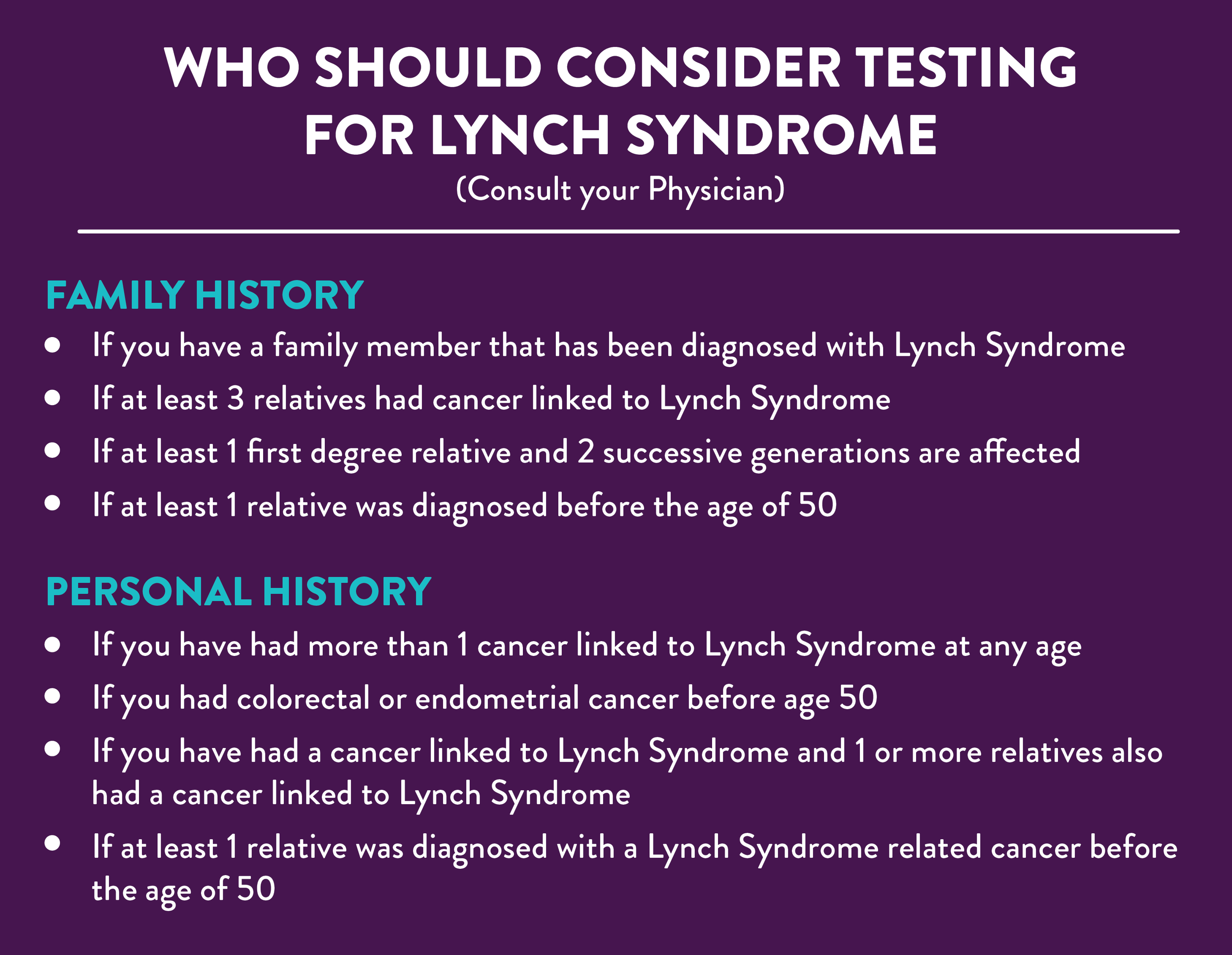
The Bethesda criteria help clinicians decide when to test tumors for mismatch repair (MMR) deficiencya hallmark of Lynch syndrome. Key triggers include: colorectal cancer diagnosed before age50, multiple primary cancers, or a family history that fits the Amsterdam criteria.
When to test even without criteria?
If you have a known pathogenic mutation in your family, you should be offered testing regardless of the Bethesda rules. Likewise, if you have a strong personal or family cancer history that doesnt fit neatly into the list, a discussion with a genetics counselor is worthwhile.
Balancing Benefits & Risks
The upside of regular screening
Early detection dramatically improves survival rates. For colon cancer, a stageI diagnosis has a 90%+ fiveyear survival, compared to under 20% for stageIV. Regular endoscopies also let doctors remove polyps before they turn malignanta true lifesaver.
The downsides to consider
Procedures arent riskfree. Colonoscopies carry a small chance of perforation (about 1 in 10,000) and bleeding, especially after polyp removal. Repeated anesthesia can cause mild fatigue. Moreover, falsepositive findings may lead to unnecessary anxiety or additional tests.
ProsandCons Snapshot
| Benefit | Risk |
|---|---|
| Detects cancers early higher cure rates | Procedural discomfort and rare complications |
| Removes precancerous polyps prevents cancer | Potential falsepositive results extra testing |
| Provides peace of mind | Possible anxiety from frequent testing |
Action Plan: Getting Started Today
Stepbystep checklist
- Confirm your genetic status. If you havent been tested, schedule a blood or saliva test.
- Find a genetics counselor. Theyll interpret results and tailor the surveillance schedule.
- Set up your first colonoscopy. Aim for the age recommended for your specific gene.
- Ask about upperGI endoscopy. Even if you feel fine, early screening can be a gamechanger.
- Arrange gynecologic surveillance. Women should discuss endometrial biopsies with their OBGYN.
- Check insurance coverage. Use tools like the American Cancer Society cost estimator to anticipate outofpocket fees.
- Keep a tracking calendar. Mark each appointment, test result, and followup date.
Free printable calendar
Ive put together a simple PDF you can download, print, and hang on your fridge. It lists colonoscopy, upperGI, and gynecologic dates based on the most common guideline timelines. (Imagine a friendly reminder that says, Hey, its time for your next checkuplets keep you healthy!)
Conclusion
Sticking to the lynch syndrome screening guidelines isnt just a medical choreits a proactive way to protect yourself and your loved ones. By beginning colonoscopies in your 20s, adding upperGI endoscopy in your 30s, and staying on top of gynecologic checks, you create a robust safety net that catches problems early. Remember, the best defense is a wellplanned offense: schedule that first appointment, talk to a genetics professional, and use the resources at hand. Youve got the knowledge, the tools, and a supportive community behind youso go ahead and take that next step with confidence. If anything feels overwhelming, reach out to a trusted health provider; theyre there to help you navigate the path forward.
For related reading on cancer nutrition while undergoing surveillance, consider a practical guide to a Cancer diet plan that many patients find helpful alongside regular screening.
FAQs
What are the main Lynch syndrome screening guidelines?
The main guidelines recommend regular colonoscopies starting in your 20s, upper GI endoscopy in your 30s, and gynecologic checks for women beginning at age 30–35.
When should colonoscopy screening start for Lynch syndrome?
Colonoscopy should start at age 20–25 for MLH1/MSH2 carriers, 30 for MSH6, and 35 for PMS2, with repeat exams every 1–2 years.
What tests are used for Lynch syndrome screening?
Screening includes colonoscopy, upper GI endoscopy, endometrial biopsy, and genetic testing for MMR deficiency or MSI.
Are there special guidelines for women with Lynch syndrome?
Women should have annual endometrial biopsies or transvaginal ultrasounds starting at age 30–35, and discuss gynecologic surveillance with their doctor.
How often should Lynch syndrome screening be done?
Colonoscopy is recommended every 1–2 years, upper GI endoscopy every 3–5 years, and gynecologic checks annually or as advised by your healthcare provider.