Getting diagnosed with Kaposi sarcoma can feel like stepping onto a rollercoaster you never signed up for. The good news? There are many ways to manage the disease, and the right plan depends on where you are, how your immune system is doing, and what matters most to you. Below youll find a friendly, downtoearth rundown of the main treatments, how doctors decide whats best, and where to find reliable resources that actually help.
Understanding Kaposi Sarcoma
What is Kaposi sarcoma?
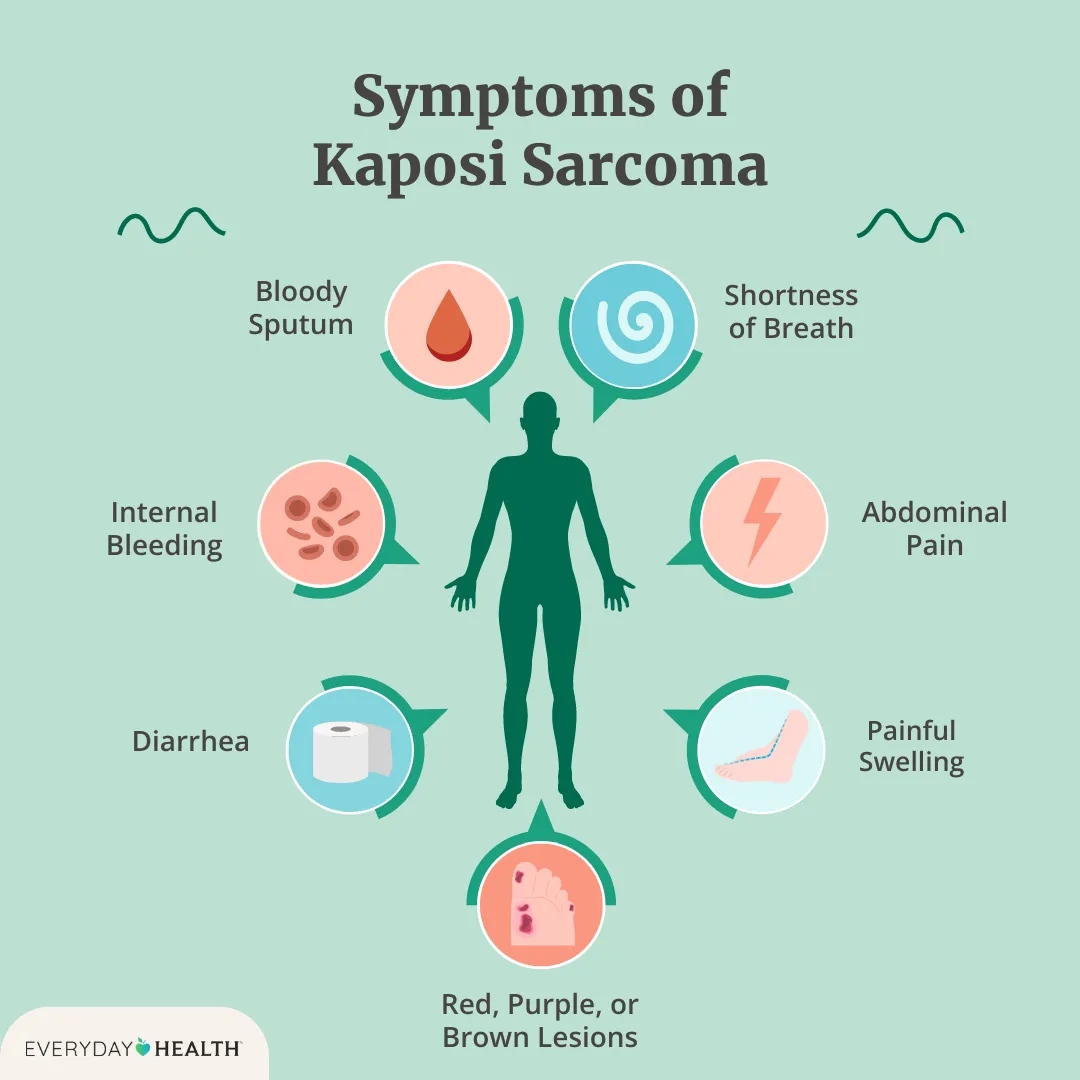
Kaposi sarcoma (KS) is a type of cancer that starts in the cells lining blood vessels and lymphatics. It shows up as reddishpurple spots on the skin, but it can also affect internal organs. The culprit behind most cases is a virus called human herpesvirus8 (HHV8). When the immune system is weakenedespecially in people living with HIVthe virus can run wild, leading to those characteristic lesions.
Types & why treatment differs
There are four recognized forms:
- Epidemic (HIVrelated) most common in people with HIV.
- Classic usually slowgrowing, often seen in older Mediterranean men.
- Iatrogenic triggered by immunosuppressive drugs after organ transplants.
- Endemic occurs in parts of Africa where HHV8 is widespread.
Because each type behaves differently, the treatment plan is tailored to the specific form, the extent of disease, and the patients overall health.
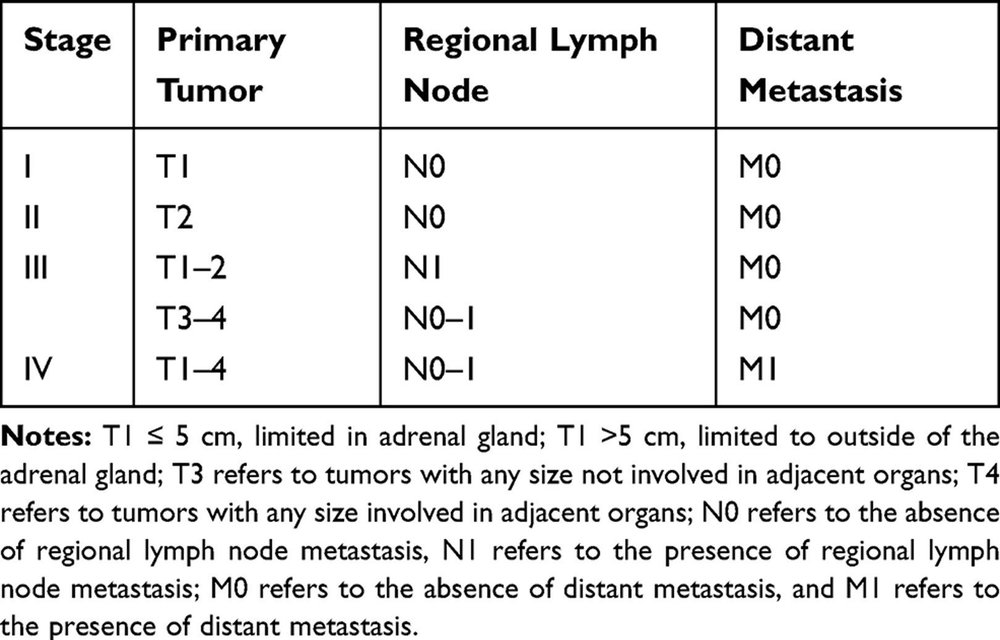
How clinicians stage the disease
Staging looks at three main things: the number and size of skin lesions, whether internal organs are involved, and in HIVpositive patients, the CD4 count and viral load. This information helps doctors pick the safest, most effective approach.
EEAT tip
When you write the full article, pull the latest staging table from the (NCI) and quote it directly. Adding a short vignettelike a 38yearold man with a CD4 count of 180cells/Lwill make the information feel real and trustworthy.
Treatment Options Overview
| Modality | When Used | Main Benefit | Key Risks / SideEffects |
|---|---|---|---|
| Local therapies (cryotherapy, excision, radiation) | 10 skin lesions, no internal disease | Fast cosmetic control, minimal systemic exposure | Scarring, pigment changes, pain |
| Systemic chemotherapy (liposomal doxorubicin, paclitaxel) | Diffuse cutaneous or visceral disease, rapid progression | High response rates, diseasecontrol | Myelosuppression, cardiotoxicity, neuropathy |
| Immunomodulation (ART for HIV, interferon) | HIVpositive or immunedeficient patients | Restores immune surveillance, can shrink lesions | Flulike symptoms, liver toxicity |
| Targeted agents (thalidomide, VEGF inhibitors) | Refractory cases, clinicaltrial setting | Oral, less intense than chemo | Neuropathy, thrombosis, teratogenic risk |
| Supportive care (pain control, wound management) | All stages | Improves quality of life | Medication sideeffects |
Local Treatment Details
If you have only a handful of lesions, a quick outpatient procedure can do the trick. Cryotherapy freezes the spot, curing it in a single visit. Radiation, on the other hand, is great for thicker plaques or lesions in hardtoreach spots like the mouth.
Stepbystep Cryotherapy Checklist
- Confirm lesion size (1cm is ideal).
- Apply liquid nitrogen for 1015seconds.
- Allow the area to thaw; repeat once if needed.
- Cover with a sterile dressing for 24hours.
Systemic Chemotherapy Protocols
When KS spreads beyond the skin, doctors often turn to chemo. The most widely used regimen is liposomal doxorubicin20mg/m IV every 23weeks. If you cant tolerate that, paclitaxel (100mg/m weekly for three weeks, then a week off) is a solid alternative.
Managing SideEffects
Neutropenia (low whiteblood cells) is the most common snag. The recommends growthfactor support when counts dip below 1,000L. Keep a symptom diary and let your nurse know about any fevers right away.
HIVRelated Treatment (Kaposi sarcoma in HIV)
For people living with HIV, the first line is always antiretroviral therapy (ART). Getting the virus under control often makes KS shrink on its own. However, when lesions are aggressive, adding chemo on top of ART is the standard of care.
Realworld story
Maria, 32, was diagnosed with HIVrelated KS after noticing purple patches on her legs. Within three months of starting a modern ART regimen and receiving just two cycles of liposomal doxorubicin, most of her lesions faded dramatically. She says the biggest surprise was how quickly her energy returned once the virus was suppressed.
Emerging & Experimental Options
Researchers are testing oral agents like thalidomide and lenalidomide, as well as VEGF inhibitors such as bevacizumab. While promising, these are usually reserved for patients who have already tried standard chemo.
Topical Retinoids
In some limitedskin cases, doctors prescribe alitretinoin cream. It works slowly but can be a gentle alternative for people who cant tolerate injections.
Choosing the Right Plan
Decisionmaking checklist
- Is the disease local or systemic?
- Are you HIVpositive? Whats your CD4 count?
- Do you have heart, liver, or kidney concerns?
- How often can you travel for infusions?
- What cosmetic outcome matters most to you?
Questions to ask your oncologist
- What response rate can I expect from this regimen?
- How will this interact with my HIV meds?
- What labs will you check and how often?
Comparison: Local vs. Systemic vs. Targeted
| Approach | Pros | Cons | Typical Cost (US$) | Visit Frequency |
|---|---|---|---|---|
| Local (cryotherapy, radiation) | Quick, minimal systemic impact | Limited to few lesions, possible scarring | 1,0003,000 | 12 visits |
| Systemic chemo | Effective for widespread disease | Sideeffects, infusion center visits | 5,00012,000 per cycle | Every 23 weeks |
| Targeted agents | Oral, less intense than chemo | Limited data, may cause neuropathy | 8,00015,000 per year | Daily oral |
Trusted Resources & Guides
Official PDFs & Guidelines
For the most uptodate, evidencebased recommendations, download the from the NCI. It walks you through staging, drug dosing, and followup schedules in plain language.
Reliable PatientFacing Sites
Websites like and the break down each option without the jargon overload.
Support Communities
Connecting with others can be a lifeline. The Kaposi Sarcoma Foundation runs online forums where patients share treatment experiences, and the AIDS Cancer Consortium often posts webinars about the newest drug combos.
How to verify a medical PDF
- Check the URL ends in
.govor.org. - Look for a recent revision date (ideally within the past 2 years).
- Confirm authorshipclinical experts, not marketing teams.
Monitoring & FollowUp
Posttreatment surveillance schedule
- Skin exam every 3months for the first year, then every 6months.
- CD4 count & viral load every 23months if youre HIVpositive.
- Imaging (CT or PET) only if you had visceral involvement at diagnosis.
Signs of recurrence to watch for
New purple patches, swelling in the limbs, oral lesions, or unexplained shortness of breath should prompt a quick call to your oncology team.
Quickreference flowchart (text version)
Remission Routine check Early detection Retreat or switch therapy
Lifestyle & Support
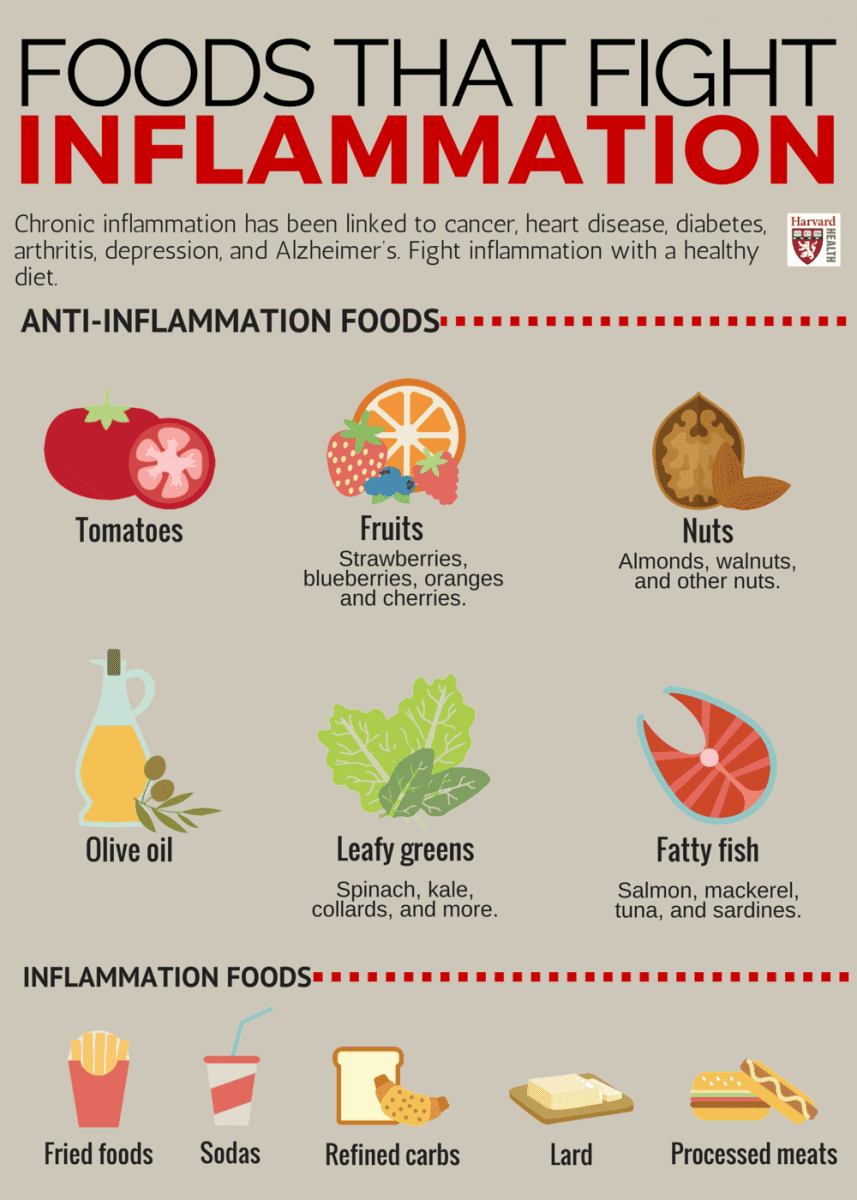
Nutrition, exercise, and immune health
Eating a balanced diet rich in protein, fresh fruits, and veggies gives your immune system the fuel it needs. A daily 30minute walk or gentle yoga can also boost circulation, which may help lesions heal faster.
Coping with the emotional impact
Its normal to feel scared, angry, or even guilty. Talking to a counselor, joining a peersupport group, or practicing mindfulness can ease the emotional load. Remember, youre not alonemany have walked this path and emerged stronger.
Top 5 apps & forums for KS patients
- MyHealthTeams a community for people living with KS.
- HealtheLife secure messaging with your care team.
- Insight Timer guided meditations for stress relief.
- SimplePractice for tracking symptoms and meds.
- Reddits r/HIVSupport realworld advice from peers.
Conclusion
Kaposi sarcoma treatment isnt a onesizefitsall prescription. By understanding the different disease types, weighing the pros and cons of local versus systemic options, and staying on top of followup care, you can shape a plan that fits your life and health goals. Grab the latest , talk openly with your oncologist, and lean on trusted support networks. You deserve a treatment journey thats as thoughtful and hopeful as you are. If you have questions or want to share your own story, drop a comment belowlets keep the conversation going.
FAQs
What are the first‑line treatments for Kaposi sarcoma?
For HIV‑related Kaposi sarcoma, starting antiretroviral therapy (ART) is the primary step. If lesions are extensive or rapidly progressing, clinicians add systemic chemotherapy such as liposomal doxorubicin or paclitaxel.
When is local therapy like cryotherapy appropriate?
Local treatments are best when there are ten or fewer skin lesions with no internal organ involvement. Cryotherapy, excision, or radiation can quickly remove or shrink individual lesions while avoiding systemic side‑effects.
How does a patient’s CD4 count affect treatment decisions?
A lower CD4 count (especially below 200 cells/µL) indicates a weakened immune system. In such cases, restoring immune function with ART becomes critical, and clinicians may choose less aggressive chemotherapy regimens to minimize infection risk.
What side‑effects should I expect from liposomal doxorubicin?
Common side‑effects include neutropenia (low white‑blood cells), mild nausea, and fatigue. Rarely, patients may experience cardiotoxicity, so heart function is monitored before and during treatment.
Are there any oral or targeted drugs for Kaposi sarcoma?
Yes. Oral agents like thalidomide and lenalidomide, as well as VEGF inhibitors such as bevacizumab, are used in refractory cases or clinical trials. They are generally less intense than traditional chemotherapy but can cause neuropathy or increased clotting risk.