Quick Start Overview
What are the IDSA meningitis guidelines?
The Infectious Diseases Society of America (IDSA) puts together evidencebased, peerreviewed recommendations for diagnosing and treating meningitis. Think of them as a trusted road map for clinicians navigating the fastmoving terrain of bacterial, viral, and healthcareassociated infections.
Where can I download the latest PDFs?
Getting the official documents is easy. The IDSA site hosts the most recent versions, and you can grab them with a single click:
| Year | PDF Link | File Size |
|---|---|---|
| 2024 | 2.3MB | |
| 2023 | 2.1MB | |
| 2021 | 2.0MB |
Why keep older versions?
Older PDFs serve as a historical baseline. Seeing how recommendations have shifted helps you understand the why behind each change, especially when youre discussing treatment plans with colleagues or trainees.
Guideline Authority
The IDSA development process
The guidelines arent pulled out of thin air. A multidisciplinary panelinfectiousdisease physicians, pediatric neurologists, epidemiologists, and pharmacistsconducts systematic reviews, grades evidence using the GRADE system, and drafts statements that undergo multiple rounds of peer review.
Key panel members and credentials
Names like Dr.Emily Chen (MD, PhD, pediatric infectiousdisease specialist) and Dr.Mark Rivera (MD, senior IDSA fellow) appear on the author list. Their combined experience spans decades, from bedside care in tertiary hospitals to research on antimicrobial resistance.
Expert insight (optional)
The 2024 update reflects growing data on ESBLproducing organisms, notes Dr.Rivera in a recent interview. It pushes us to think beyond the classic ceftriaxoneplusvancomycin combo for certain highrisk patients.
Diagnostic Recommendations
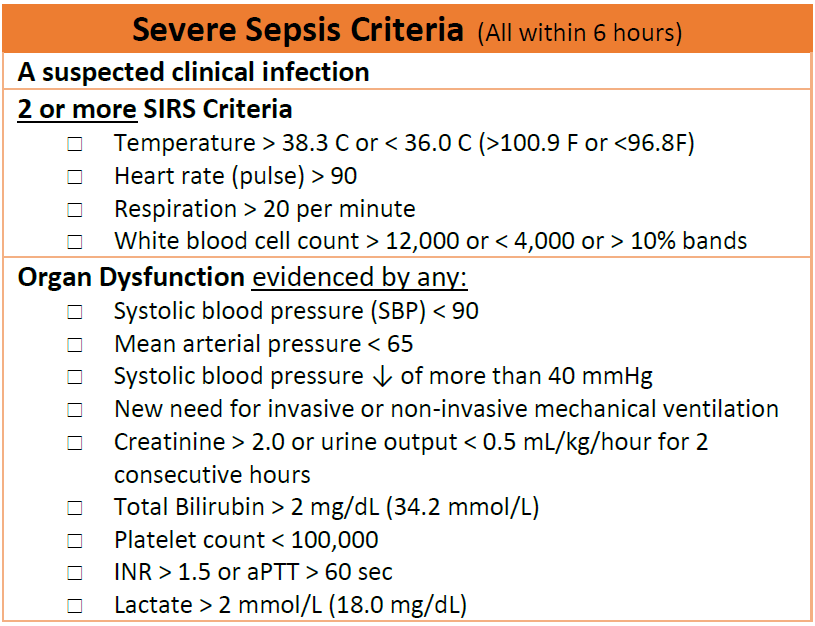
How does IDSA define suspected bacterial meningitis?
Any patient with acute fever, neck rigidity, altered mental status, or a newonset seizure should raise the red flag. The guideline stresses that suspicion alone warrants empirical therapy, because waiting for culture results can cost lives.
What CSF findings trigger treatment?
Typical bacterial CSF shows:
- Whiteblood cell count >1,000cells/L (predominantly neutrophils)
- Protein >100mg/dL
- Glucose <40mg/dL or <40% of serum glucose
If you see two of these three, start antibiotics immediately.
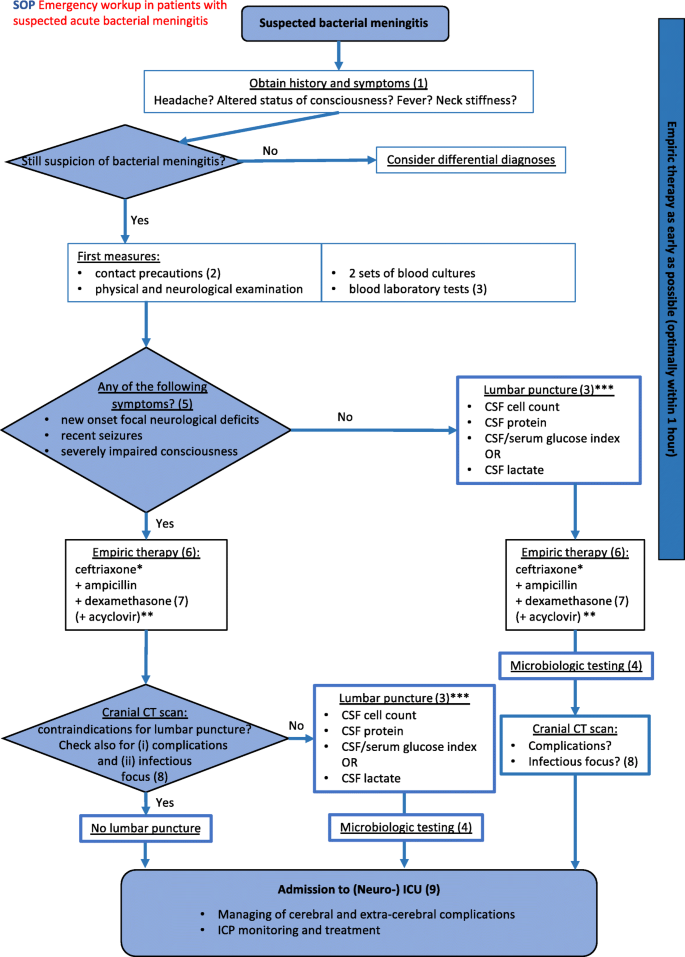
When are imaging studies required before LP?
Before you pull a lumbar puncture, check for signs of raised intracranial pressurefocal neurologic deficits, papilledema, or a sudden, severe headache. In those cases, a CT scan first is nonnegotiable.
Decisiontree (quick visual)
Symptom onset Evaluate for redflag signs (If none) Perform LP Start empiric antibiotics Adjust based on CSF results.
Treatment Recommendations
Firstline antibiotics for adults (2024)
The current adult regimen is:
- Vancomycin 1520mg/kg IV every 812h (target trough 1520g/mL)
- Ceftriaxone 2g IV every 12h or cefepime 2g IV every 8h if ESBL risk is high
These cover the usual suspectsStreptococcus pneumoniae, Neisseria meningitidis, and Haemophilus influenzaewhile guarding against resistant strains.
Firstline antibiotics for children (pediatric meningitis guidelines)
For kids, the regimen swaps ceftriaxone for cefotaxime (due to better CSF penetration) and adds ampicillin when Listeria risk is present (infants <1month or immunocompromised).
- Vancomycin 15mg/kg IV q6h
- Cefotaxime 50mg/kg IV q6h
- Ampicillin 200mg/kg IV q4h (if indicated)
Adjunctive steroids: timing and dosing
Dexamethasone 0.15mg/kg IV (max 10mg) given just before or with the first antibiotic dose cuts inflammationmediated damage, especially in pneumococcal meningitis. The guideline emphasizes give it early, or dont give it at all.
Dosing tables
| Group | Drug | Dose | Frequency |
|---|---|---|---|
| Adult | Vancomycin | 1520mg/kg | q812h |
| Adult | Ceftriaxone | 2g | q12h |
| Pediatric | Cefotaxime | 50mg/kg | q6h |
| Pediatric | Ampicillin | 200mg/kg | q4h |
Common druginteraction warnings
Vancomycin and aminoglycosides together can increase nephrotoxicity. If you need both, monitor creatinine closely and adjust dosing as needed.
Special Populations
Pediatrics
Kids arent just small adults. Their immune systems and vaccine histories shift the microbial landscape. The guidelines stress broader coverage for Listeria in newborns and for Haemophilus influenzae typeb in unvaccinated toddlers.
Viral meningitis & IDSA viral meningitis guidelines
If PCR shows a virus (enterovirus, HSV1, or VZV), antibiotics are usually stopped after 24hours of observation. Supportive carefluids, analgesia, and close monitoringremains the cornerstone.
Immunocompromised & healthcareassociated cases
Patients with recent neurosurgery, ventriculostomy, or prolonged ICU stays need a broader spectrumoften adding meropenem or linezolid to cover Gramnegative and resistant organisms.
Comparison table
| Condition | Empiric Regimen | Key Considerations |
|---|---|---|
| Bacterial (standard) | Vancomycin+Ceftriaxone | Coverage for S. pneumoniae & N. meningitidis |
| Viral | Supportive only | Stop antibiotics if PCR negative for bacteria |
| HCassociated | Vancomycin+Meropenem | Watch for ESBL, Pseudomonas |
2024 Updates: Benefits vs. Risks
New antimicrobial recommendations
The 2024 edition swaps ceftriaxone for cefepime in settings where ESBLproducing Enterobacteriaceae are common. This adds broader Gramnegative coverage but also raises the risk of neutropeniaso regular CBC checks are advised.
Revised steroid timing
Earlier data suggested a within 15minutes window for dexamethasone. The updated guideline relaxes this slightly to before or with the first dose, acknowledging realworld workflow constraints while retaining benefit.
What older clinicians should watch for
If you still reference the 2021 PDF, be wary of the nowoutdated vancomycin trough target (1015g/mL) and the lack of cefepime as an alternative. Those discrepancies can lead to suboptimal therapy.
Sidebyside comparison (2021 vs. 2024)
| Feature | 2021 | 2024 |
|---|---|---|
| Primary Gramnegative coverage | Ceftriaxone | CeftriaxoneorCefepime (ESBL risk) |
| Vancomycin trough goal | 1015g/mL | 1520g/mL |
| Dexamethasone timing | Within 15min | Before/with first antibiotic |
Practical Tools for Busy Clinicians
Printable cheatsheet
Weve distilled the key points into a onepage PDF you can stash in your pocket or EMR toolbar. It lists dosing, timing, and redflag checksall in less than a minute to glance at.
Mobile app/website quickreference
The IDSA practiceguideline portal offers a responsive design that works on phones and tablets. Simply tap Meningitis and youre looking at the full algorithm, downloadable PDFs, and a builtin calculator for weightbased dosing.
Integrating the guideline into EMR order sets
Most hospitals now allow custom order panels. By creating a Meningitis Bundle that autopopulates vancomycin, ceftriaxone (or cefepime), dexamethasone, and a CSF lab panel, you shave minutes off the critical timetofirstdose metric.
Sample EMR order set screenshot (description)
Imagine an order screen with four columns: Medication, Dose, Frequency, and Comments. The first row reads Vancomycin 15mg/kg q12h Target trough 1520g/mL. The next rows follow for ceftriaxone/cefepime, dexamethasone, and a CSF lab bundle.
Sources & Trustworthiness
Primary IDSA documents
All recommendations are drawn directly from the official and its archived PDFs for 2023 and 2021.
Peerreviewed summary article
A 2024 review in Clinical Infectious Diseases validates the GRADE methodology and highlights the clinical impact of the new cefepime option.
Complementary resources
The CDCs meningitis fact sheet offers epidemiologic context and vaccination recommendations, useful for patient education. (Reference: CDC meningitis overview, 2024.)
Suggested citation format
American Society of Infectious Diseases. (2024). Clinical Practice Guidelines for the Management of Bacterial Meningitis. IDSA.
Conclusion
The IDSA meningitis guidelines are more than a checklisttheyre a lifeline for clinicians at the bedside. By grabbing the , familiarizing yourself with the diagnostic triggers, applying the updated antibiotic and steroid regimens, and using the handy cheatsheet, youll feel prepared to act swiftly and responsibly.
Remember, the balance between benefit (saving a life, reducing neurologic sequelae) and risk (antibiotic toxicity, resistance) is delicate but manageable when you follow the evidencebased pathway. Download the tools, integrate them into your workflow, and stay curiousmedicine evolves, and so should we. If youve faced a meningitis case, share what worked for you, or ask any lingering questions. Together we keep patients safe and informed.
For quick reference on appropriate antibiotic choices in severe infections and to review examples of recommended agents, see meningitis antibiotics for concise dosing examples and selection considerations.
FAQs
What are the IDSA meningitis guidelines?
The IDSA meningitis guidelines are evidence-based recommendations for diagnosing and treating bacterial meningitis, updated regularly for best clinical practice.
When should empiric antibiotics be started for suspected meningitis?
Empiric antibiotics should be started immediately if bacterial meningitis is suspected, even before confirmatory tests, to reduce risk of complications.
What is the first-line antibiotic regimen for adults with meningitis?
For adults, the first-line regimen is vancomycin plus ceftriaxone or cefepime, depending on local resistance patterns and patient risk factors.
Are steroids recommended in meningitis treatment?
Dexamethasone is recommended for pneumococcal meningitis, given just before or with the first antibiotic dose to reduce inflammation and complications.
How do the guidelines differ for pediatric meningitis?
Pediatric guidelines recommend cefotaxime instead of ceftriaxone and add ampicillin for infants or immunocompromised children to cover Listeria.