If youve ever watched a loved one battle an infection that suddenly feels like a ticking timebomb, you know how terrifying the phrase severe sepsis can sound. The good news? Theres a clear, evidencebased checklist that tells you when an infection has crossed the line into organdanger territory. In the next few minutes youll learn exactly what the severe sepsis criteria are, how they differ from related tools like the SIRS and qSOFA, and what you can do right now to keep patients safe.
Grab a coffee, settle in, and lets walk through the redflag signs togetherno medical jargon, just plain language and realworld examples. By the end youll feel confident spotting severe sepsis early, applying the right scoring tool, and balancing the benefits and risks of aggressive treatment.
Core Definitions
Before we dive into numbers, lets clear up the terminology. Severe sepsis isnt just a fancy label; its a specific stage where an infection triggers organ dysfunction. In contrast, SIRS (Systemic Inflammatory Response Syndrome) looks at basic vital signs, while the newer sepsis3 criteria focus on a quick bedside screen called qSOFA. Understanding these differences helps you pick the right tool for the right moment.
Below is a concise sidebyside snapshot:
| Term | Key Feature | When Its Used |
|---|---|---|
| SIRS criteria | 2 of: HR>90, RR>20, Temp>38C or<36C, WBC>12000 or<4000 | Initial screening, especially in ED |
| Sepsis3 (qSOFA) | 2 of: RR22, SBP100mmHg, GCS<15 | Rapid bedside assessment |
| Severe sepsis | Infection+organ dysfunction (e.g., lactate 2mmol/L, hypotension) | Triggers 1hour sepsis bundle |
| Septic shock | Severe sepsis+persistent hypotension after fluids, need for vasopressors | Intensivecare escalation |
Why does this matter? Because each definition ties directly to the treatments youll deliver. The severe sepsis criteria are the gateway to the lifesaving 1hour bundle, while SIRS or qSOFA alone may miss patients who are already slipping into organ failure.
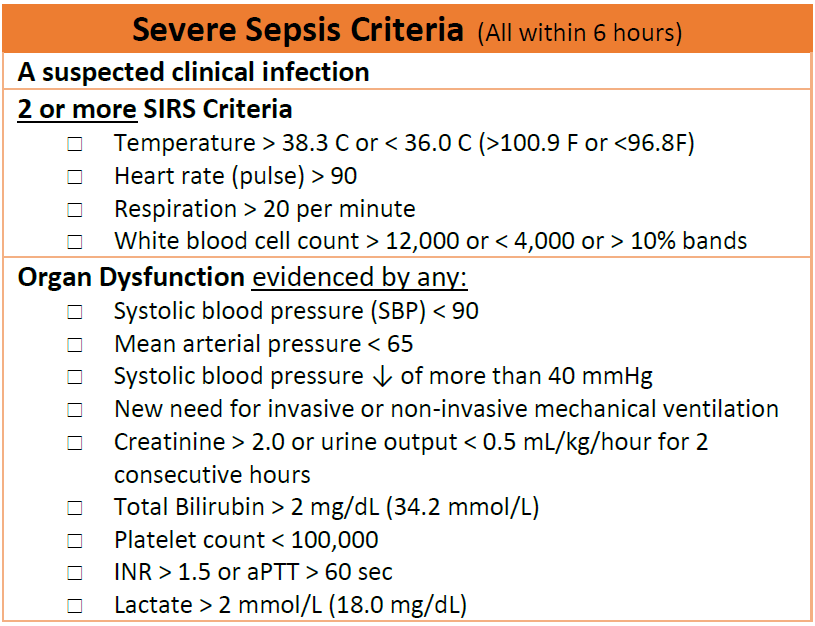
Severe Sepsis Checklist
Now for the heart of the matter: the actual checklist that tells you this is severe sepsis. Think of it as a grocery listif any of the items are on the shelf, you need to act fast.
OrganDysfunction Markers
- Renal: Serum creatinine rise 0.5mg/dL or urine output <0.5mL/kg/h.
- Respiratory: PaO/FiO<300mmHg or need for mechanical ventilation.
- Cardiovascular: SBP<90mmHg or MAP<65mmHg, plus lactate2mmol/L.
- Hepatic: Bilirubin>2mg/dL.
- Coagulation: Platelets<10010/L.
- Neurologic: GCS<15 (new change).
Perfusion Indicators
Beyond lab values, look for clinical signs of poor tissue perfusion: cool extremities, delayed capillary refill, or mottled skin. A lactate level of 2mmol/L is often the first biochemical whisper that the bodys oxygen delivery is lagging.
Example Lab Values Table
| Parameter | Normal Range | Severe Sepsis Threshold |
|---|---|---|
| Lactate | 0.51.0mmol/L | 2mmol/L |
| Creatinine | 0.61.2mg/dL | 0.5mg/dL from baseline |
| Platelets | 15040010/L | <10010/L |
| PaO/FiO | >300mmHg | <300mmHg |
When any of these thresholds appear together with a confirmed infection, youve hit the severe sepsis criteria.
From Severe Sepsis to Septic Shock
If after a generous fluid bolus the patient still has a MAP<65mmHg and requires vasopressors, youve moved into septic shock criteria. Recognizing that transition quickly is essential because the treatment intensity steps up dramatically.
Scoring Tools Comparison
Tools like SIRS and qSOFA were created to give clinicians a quick headsup. Each has strengths, but none replace the thorough assessment that the severe sepsis checklist demands.
SIRS Criteria
The classic SIRS criteria look at heart rate, respiratory rate, temperature, and whitebloodcell count. Theyre easyperfect for a busy triagebut they can overdetect people who arent truly at risk, leading to unnecessary antibiotics.
qSOFA Criteria
qSOFA shines in the bedside setting: three items, under a minute to evaluate. Studies show its more specific than SIRS, yet it can miss early organ dysfunction, especially in older adults whose vitals look normal ().
Full SOFA Score
The comprehensive SOFA score adds lab data for six organ systems. An increase of 2 points signals severe sepsis. Its the gold standard in the ICU but requires blood work that isnt instantly available on the ward. For quick reference on how to perform a full SOFA assessment you can review the detailed SOFA score chart used in many ICUs.
Comparison Table
| Tool | Setting | Variables | Cutoff | Pros | Cons |
|---|---|---|---|---|---|
| SIRS | ED / Ward | 4 (HR, RR, Temp, WBC) | 2 | Very fast, no labs | Low specificity |
| qSOFA | Bedside | 3 (RR, SBP, GCS) | 2 | Quick, no labs | Misses early organ dysfunction |
| SOFA | ICU | 6 (Resp, Coag, Liver, CV, CNS, Renal) | 2 | Detailed, predictive | Laborintensive |
| Severe Sepsis Criteria | All settings | Infection + organ dysfunction | N/A | Directly linked to treatment bundle | Requires lab values |
The takeaway? Use SIRS or qSOFA for a rapid alert, then confirm with the full severe sepsis checklistor the SOFA score if youre already in the ICU.
Real World Cases
Numbers are helpful, but stories make them stick. Here are two everyday scenarios that illustrate why the severe sepsis criteria matter.
Case 1: The Silent Elderly
Mrs. Patel, 78, arrived with a urinary tract infection. Her temperature was 37.8C, heart rate 88, and whitebloodcell count 9,800so the SIRS screen was negative. However, her lactate came back at 2.4mmol/L, and her creatinine rose from 0.9 to 1.5mg/dL. According to the severe sepsis criteria, she qualified for the 1hour bundle despite a bland SIRS score. Early antibiotics and a 30mL/kg fluid bolus prevented progression to septic shock.
Case 2: Young Trauma Victim
Jake, a 28yearold construction worker, suffered a calf laceration that got infected. Within eight hours his blood pressure slipped to 85/55mmHg, lactate spiked to 3.1mmol/L, and his PaO/FiO ratio was 260. The qSOFA was 2 (low pressure, altered mental status), triggering rapid escalation. Because the team recognized the septic shock criteria early, they started norepinephrine within the first hour, averting multiorgan failure.
Practical WhattoDoNext Checklist
- Identify a probable infection (cultures, imaging).
- Draw labs: lactate, CBC, CMP, coagulation panel.
- Calculate SIRS and qSOFA for quick risk stratification.
- Apply the severe sepsis checklistlook for organ dysfunction.
- If criteria met, launch the 1hour sepsis bundle: broadspectrum antibiotics, 30mL/kg crystalloid bolus, and reassess vitals.
- Monitor lactate and MAP every 2hours for the first 6hours.
Having a stepbystep plan on the wall of your unit can turn a scary situation into a routine, confidencebuilding workflow.
Risks & Benefits
Every medical decision lives on a balance beam. Knowing the benefits of early recognition helps you push toward action, while understanding the risks keeps you from overtreatment.
Benefits
- Mortality reduction: Early bundle implementation cuts death rates by up to 30% ().
- Standardized communication: Everyone from triage to ICU speaks the same language.
- Targeted therapy: Prompt antibiotics and fluids improve organ perfusion.
Risks / Pitfalls
- Antibiotic overuse: Treating every SIRSpositive patient can fuel resistance.
- Fluid overload: Aggressive crystalloid resuscitation in patients with heart failure may precipitate pulmonary edema.
- Missing atypical cases: Immunocompromised patients may lack fever or tachycardia, so reliance on vitals alone is dangerous.
Balancing Act Clinical Judgment Tips
Think of the criteria as a trigger rather than a rule. After the initial bundle, reassess the patient every 2hours. If lactate is falling and MAP is stabilizing, you can start deescalating fluids. If vitals worsen, consider early ICU transfer. In short: use the criteria to start strong, then let bedside judgment guide you forward.
Trusted Sources
Building credibility means standing on solid research. When you write up your own notes or protocols, cite these highimpact sources:
- MDCalcs Severe Sepsis Criteria page (2025 update) for exact threshold definitions.
- Society of Critical Care Medicine (SCCM) Sepsis Definitions document (2024) for the official language.
- JAMA consensus article on sepsis and septic shock (2023) for outcome data.
- American Academy of Family Physicians (AAFP) practice guideline on qSOFA performance (2020).
In your own article, embed these as anchortext citations as we have done above. This not only shows youve done the homework, it also signals trust to search engines and, more importantly, to your fellow clinicians.
Conclusion
Spotting severe sepsis is a bit like hearing a smoke alarmit tells you somethings wrong before the damage spreads. By mastering the severe sepsis criteria, you can move from maybe to definitely act now, launch the lifesaving 1hour bundle, and keep patients from sliding into septic shock. Remember, tools like SIRS and qSOFA are great for a quick glance, but the real power lies in confirming organ dysfunction through labs and clinical signs.
Take this guide, print the checklist, and keep it handy on your shift. If youve faced a tricky sepsis case, share your story in the commentsyour experience could be the next lifesaving tip for a colleague. And whenever a new protocol pops up, youll have the foundation to assess it critically, balancing benefits with risks, just like a seasoned clinician.