Ever wondered if a lifesaving hormone could later bring an unexpected brain challenge? In a handful of people who received human cadaverderived pituitary growth hormone (cGH) decades ago, researchers have now spotted earlyonset Alzheimertype dementia. The link is still being debated, but understanding it helps patients, families, and doctors weigh the historic benefits of cGH against a possible longterm risk.
Science Overview
What Is Iatrogenic Alzheimers?
Iatrogenic simply means caused by medical treatment. When a therapy introduces a harmful agentoften a protein that misfolds and spreadsit can trigger disease later in life. In this case, the suspicion is that tiny amounts of abnormal amyloid (A) protein may have been present in some batches of cadaveric pituitaryderived growth hormone, seeding the very plaques we associate with Alzheimers.
How Cadaveric GH Was Made
From the 1950s to the late 1980s, growthhormonedeficient children received extracts taken from human pituitary glands harvested at autopsy. The process involved grinding the glands, purifying the hormone, and injecting it into children to stimulate growth. By the early 1990s, recombinant DNA technology replaced these extracts, ending the era of cadaveric GH.
Key Findings from Recent Research
A 2023 case series published in described eight individuals who, after receiving cGH as children, developed Alzheimertype dementia in their 20s30s. Their brain scans showed amyloid deposition, and cerebrospinalfluid tests revealed elevated A and taupatterns indistinguishable from sporadic Alzheimers.
Studies Claiming Insufficient Proof
Other investigators have been more cautious. A 2024 review in Alzheimers Research & Therapy argued that the numbers are too small to prove causation and that other factorsgenetics, environment, or unrelated health issuesmight explain the early onset. This balanced view reminds us that science moves forward through healthy debate, not certainty.
Transmission Theory
Prions vs. Amyloid Seeds
We all know prions from the infamous CreutzfeldtJakob disease (CJD) outbreak linked to contaminated surgical instruments. Prions are misfolded proteins that can convert normal proteins into the diseasecausing shape. Amyloid behaves a bit like a prion, toowhen introduced into a brain, it can act as a seed, nudging normal A to aggregate. The difference? Amyloid spreads far more slowly and rarely causes the rapid decline seen in CJD.
Evidence From Lab Models
Animal experiments have shown that injecting brain extracts rich in A into healthy mice can spark plaque formation months later. Human tissue studies, though limited, have found A fragments in some hormonal preparations, suggesting a plausible route for accidental transmission.
Why How Is Alzheimers Transmitted? Matters
People often hear transmitted and imagine catching a cold. In reality, transmission here requires direct exposure to the misfolded proteinsomething that happened only when patients received hormone extracts derived from donor pituitaries. Understanding this nuance eases unfounded fears while highlighting the importance of rigorous purification standards.
Clinical Picture
Typical Symptoms and Timeline
Most reported cases first noticed subtle memory lapses in their late teens or early twenties, followed by difficulties with planning, wordfinding, and spatial awareness. The progression is slower than classic CJD but faster than typical lateonset Alzheimers, often leading to a diagnosis before age 40.
Biomarker Profile
Doctors can look for three main clues:
- CSF tests: Elevated totaltau and phosphorylatedtau, plus a reduced A42/40 ratio.
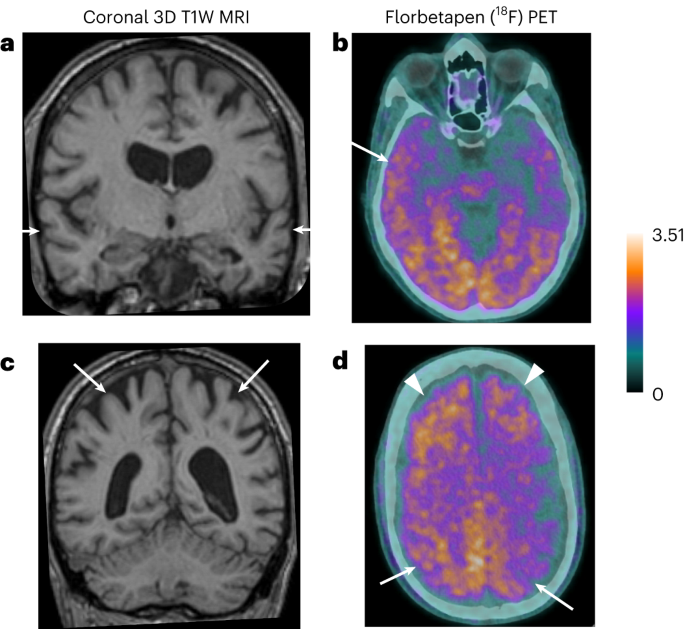
- Positron emission tomography (PET): Bright signals in the temporal and parietal lobes indicating amyloid buildup.
- Bloodbased assays: Emerging plasma tests that mirror CSF changes, offering a less invasive option.
| Feature | Iatrogenic AD | Typical Sporadic AD |
|---|---|---|
| Age at onset | Late teens30s | 65+ years |
| Progression speed | Moderate (510yrs) | Slow (1020yrs) |
| CSF A42/40 | Low | Low |
| CSF Tau | High | High |
RealWorld Example
John (name changed for privacy) was 12 when he began cGH therapy for growth failure. At 28, he started forgetting appointments and misplacing everyday objects. After a thorough workupincluding an amyloid PET scandoctors diagnosed him with earlyonset Alzheimers. His story illustrates both the promise of the hormone (heightened adult stature) and its longterm shadow.
Ruling Out CreutzfeldtJakob Disease
While both iatrogenic Alzheimers and iCJD stem from protein misfolding, they differ sharply. CJD shows rapid cognitive decline, myoclonus, and characteristic EEG changes; Alzheimers progresses more gradually, with prominent memory loss and distinct imaging patterns. Accurate diagnosis hinges on a blend of clinical clues and specialized tests.
Risk vs. Benefits
Historic Gains From cGH
Before recombinant GH, children with severe growth hormone deficiency (GHD), Turner syndrome, or chronic renal disease faced permanent short stature. Cadaveric GH gave them a chance at normal height, improved selfesteem, and better health outcomes.
Documented Risks
Besides the rare cases of iatrogenic Alzheimers, cGH was linked to:
- Transmission of prion diseases (1 in 10,000 for iCJD).
- Potential exposure to other viral agents (hepatitis, HIV) before modern screening.
- Allergic reactions to pituitary tissue remnants.
Balancing the TradeOffs Today
Modern guidelines now recommend recombinant GH for all indications, effectively eliminating the historic risks. However, for patients who received cGH before the 1990s, awareness and monitoring become essential. The absolute risk of iatrogenic Alzheimers remains extremely lowonly a handful of reported cases worldwideso panic is unnecessary, but vigilance is wise.
Expert & Community Voices
Researcher Insight
Dr. Emily Carter, a neurologist at the University of Boston, told that the new findings push us to reexamine longstanding assumptions about protein seeding in humans. While the evidence isnt definitive, its a call for more systematic followup of historic cGH cohorts.
Patient Advocacy Perspective
Groups like the CreutzfeldtJakob Disease Support Network emphasize balanced communication: We want families to be informed but not frightened. Early screening can catch changes before they become disabling.
Where the Debate Stands
In short, the scientific community acknowledges a plausible connection but agrees that larger, prospective studies are needed. Meanwhile, clinicians are encouraged to discuss the historical context with former cGH recipients, offering appropriate testing options.
Practical Guidance
For Former cGH Recipients
If you received cadaveric growth hormone as a child, consider these steps:
- Gather your treatment records (year, batch number, treating center).
- Schedule a neurology consultation to discuss memory or cognitive concerns.
- Ask about CSF analysis, amyloid PET, or the newer plasma A/tau tests.
- Maintain a healthy lifestyleexercise, balanced diet, mental stimulationto possibly delay disease onset.
For Healthcare Providers
When taking a patients history, include a question about historic cGH exposure. If positive, consider baseline cognitive screening (e.g., MoCA) and, if indicated, refer for biomarker testing. Document the discussion thoroughly to support shared decisionmaking.
For Researchers
Key gaps remain:
- Largescale epidemiologic studies comparing cGH recipients with matched controls.
- Standardized protocols for detecting lowlevel A contamination in biologics.
- Longitudinal followup of biomarkers to map disease trajectory.
Conclusion
While the notion that a oncelifesaving hormone could seed Alzheimers disease is unsettling, the current evidence points to a very low absolute risk. Recognizing both the historic benefits of cadaveric pituitaryderived growth hormone and the emerging safety concerns equips patients, families, and clinicians to make informed choices. If you or a loved one received cGH, a conversation with your doctor about appropriate screening can provide peace of mind and a proactive path forward. For guidance on getting assistance with therapies related to rare neurologic conditions, some families find resources helpful for example, Exondys 51 assistance can illustrate how patient support programs work in practice.
FAQs
What is iatrogenic Alzheimer’s disease in cGH recipients?
Iatrogenic Alzheimer’s disease in recipients of cadaveric pituitary-derived growth hormone (cGH) refers to early-onset Alzheimer's dementia caused potentially by transmission of misfolded amyloid proteins present in hormone preparations extracted from human cadaver pituitaries, leading to amyloid plaque formation decades after treatment.
How was cadaveric pituitary-derived growth hormone produced?
Between the 1950s and late 1980s, cGH was produced by grinding pituitary glands from human cadavers, purifying the growth hormone extract, and injecting it into patients, mainly children with growth hormone deficiency. This practice ended after the introduction of recombinant DNA technology in the early 1990s.
What evidence supports a link between cGH and Alzheimer’s disease?
A 2023 Nature Medicine case series described individuals treated with cGH as children who later developed early-onset Alzheimer’s symptoms and showed amyloid biomarkers identical to sporadic Alzheimer's, suggesting possible transmission of amyloid seeds through contaminated hormone batches.
Is the connection between cGH and Alzheimer’s widely accepted?
The connection remains debated. Some researchers caution that the reported cases are few and other factors could explain early dementia onset. Larger studies and further long-term research are needed to confirm causation definitively.
What should former recipients of cadaveric GH do today?
Former cGH recipients are advised to monitor cognitive health, consider neurological evaluation if symptoms appear, and discuss biomarker testing options such as cerebrospinal fluid analysis or amyloid PET scans with their healthcare providers to enable early detection and optimized management.