Are you suddenly gaining weight even though you haven't changed what you eat? Do you feel a relentless hunger that no diet seems to curb? Those are the hallmark signs of hypothalamic obesity symptoms. In the next few minutes we'll walk through what to look for, why it happens, and what you can actually do about itall in a friendly, down-to-earth way.
Core Symptoms
What is the most common sign?
Rapid, unexplained weight gain
People with hypothalamic obesity often see a sudden rise in body weightsometimes more than 5% of their total weight in under six months. It's not the slow-creep you'd expect from a typical lifestyle change; it feels like the scale is plotting against you.
How does uncontrolled hunger look?
Persistent hyperphagia
Imagine a pressure cooker that never lets off steam. You might find yourself reaching for snacks every few minutes, feeling food-obsessed, or even stealing food when no one is looking. This constant craving isn't just a lack of willpowerit's a signal from a damaged hypothalamus.
Is a low metabolic rate a symptom or a cause?
Low basal metabolic rate (BMR)
The hypothalamus acts like the body's thermostat for energy. When it's injured, the thermostat breaks, and your BMR can drop dramatically. That means you burn fewer calories at rest, making every bite count twice as much.
Are mood changes part of the picture?
Irritability and anxiety around food
When hunger never quits, frustration follows. Many report feeling on edge, short-tempered, or anxious whenever meals aren't at hand. It's a psychological ripple effect of the physiological imbalance.
Do activity levels shift?
Reduced spontaneous movement
Even simple tasks like walking to the kitchen feel exhausting. A sense of fatigue and a "lazy-body" feeling are common, especially in children who once loved playing outdoors.
Do symptoms differ between kids and adults?
Child vs. adult presentations
Kids might show a sudden deviation from their growth curve, early puberty, or school-time concentration problems. Adults often notice weight-plateau despite dieting, stubborn insulin resistance, and a rising waistline that refuses to budgesometimes a sign of truncal obesity.
Why It Happens
What damage triggers hypothalamic obesity?
Tumors, surgery, and radiation
Most cases arise after a brain tumor (like a craniopharyngioma), surgical removal of that tumor, or radiation therapy that unintentionally scars the hypothalamus. Even severe head trauma can do the trick.
How does the hypothalamus disrupt appetite?
Leptin and insulin resistance
The arcuate nucleus normally reads leptin and insulin signals to tell us when we're full. Damage makes those signals jammed, so the brain keeps shouting "eat!" even when you're stocked up on energy.
What's the role of setmelanotide?
MC4R agonist therapy
Setmelanotide is a newer drug that reactivates the melanocortin-4-receptor pathway, essentially retuning the satiety switch. Clinical trials have shown meaningful weight loss in many patients, though it's not a magic bullet and requires specialist monitoring.
Are genetics involved?
Rare monogenic forms
In a small subset, mutations in the MC4R gene or related pathways can predispose you to hypothalamic obesity, even without an obvious injury. Genetic testing is rarely needed but worth mentioning for completeness.
What's the prevalence?
How common is it?
Among survivors of pediatric brain-tumor surgery, estimates range from 0.5% to 2%a tiny slice of the population but a huge impact for those affected. The numbers are lower in the general adult population, where the condition is often underdiagnosed.
How It's Diagnosed
Which clinical tests confirm it?
History, labs, and imaging
Doctors start with a detailed weight-gain chart and a look into your eating habits. Hormonal panels (leptin, insulin, cortisol) help gauge metabolic disruption. An MRI of the hypothalamic region is the gold standard to visualize any scar tissue or residual tumor.
When should you see a doctor?
Red-flag timeline
If you've gained more than 5% of your body weight in under six months and feel a relentless hunger, it's time to book an endocrinology appointment. Early detection can prevent a cascade of secondary health issues.
Which specialists are involved?
Multidisciplinary team
An endocrinologist usually leads the charge, supported by a neuro-oncologist (if a tumor is involved), a registered dietitian, and a psychologist or behavioral therapist to tackle the hyperphagic drive.
Can it be mistaken for regular obesity?
Key distinguishing factors
Standard obesity often respondsat least a bitto conventional diet and exercise. Hypothalamic obesity, however, tends to be resistant. If you've tried several evidence-based weight-loss plans with little success, the hypothalamus might be the culprit.
What role do metabolic labs play?
Assessing comorbidities
Tests such as HOMA-IR (insulin resistance), fasting glucose, and a lipid panel help gauge the risk of type-2 diabetes, fatty liver, and cardiovascular diseasecommon companions of hypothalamic obesity.
Managing Symptoms
What lifestyle tweaks actually help?
Structured meals and NEAT tricks
Because the hypothalamus won't give you the "full" signal, consistency is key. Aim for 34 balanced meals a day, each with 30% protein, 40% complex carbs, and 30% healthy fats. Sprinkle in non-exercise activity thermogenesis (NEAT) by standing while you work, pacing during phone calls, or using a small pedal-machine under the desk.
Is there a specific diet for this condition?
Hypothalamic-friendly eating plan
The goal is to blunt the insulin surge that fuels hunger. Think low-glycemic fruits (such strawberries blood sugar impact can be a useful reference), whole-grain breads, lean proteins, and plenty of fiber. Avoid ultra-processed snacks that spike blood sugar and then crash, leaving you famished again.
When are medications indicated?
Drug options and considerations
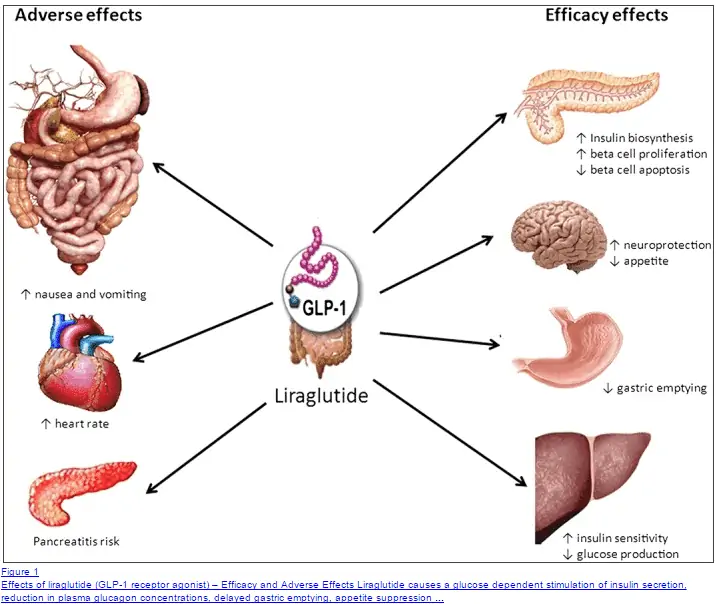
Beyond setmelanotide, doctors sometimes prescribe GLP-1 agonists (like liraglutide) to slow gastric emptying and reduce appetite. Metformin can improve insulin sensitivity, and in some cases, off-label use of appetite-suppressing agents is explored. Always discuss side-effects and costs with your specialist.
Are surgical routes an option?
Bariatric surgery outcomes
For adults with severe, refractory weight gain, bariatric surgery has shown mixed results. Some patients experience notable loss, while others see limited benefit because the underlying hypothalamic drive remains unchanged. A thorough risk-benefit analysis is essential.
How to address emotional and behavioral aspects?
Therapy and support groups
Cognitive-behavioral therapy (CBT) can reframe the relationship with food, teaching coping strategies for urges. Joining a support grouponline or in-personlets you share stories, recipes, and encouragement with people who truly get it.
What follow-up schedule works best?
Monitoring and adjusting
Quarterly lab work, semi-annual imaging, and regular weight-trend reviews keep the care plan nimble. Adjustments in medication dose, diet composition, or activity level are often needed as the body adapts.
| Treatment | Typical Use | Key Benefit | Potential Drawback |
|---|---|---|---|
| Setmelanotide | MC4R pathway activation | Significant appetite reduction | Cost, need for specialist monitoring |
| GLP-1 Agonists | Slows gastric emptying | Moderate weight loss, improves glucose | Nausea, injection burden |
| Metformin | Improves insulin sensitivity | Helps control blood sugar | GI upset in some people |
| Bariatric Surgery | Severe obesity, refractory cases | Potential large weight loss | Variable outcomes, surgical risk |
Common Questions
Can hypothalamic obesity be cured?
Control is possible, cure is rare
There's no definitive cure, but a combination of medication, diet, and behavior therapy can bring the symptoms under control and improve quality of life.
Why does weight keep rising even on a diet?
Low BMR overrides calories
When the hypothalamus tells your body it's still hungry, it also signals that you need to conserve energy. Calories you cut are often burned slower than you expect.
Is setmelanotide the miracle drug?
Effective but not universal
Setmelanotide works well for many, especially those with specific genetic pathways, but it's not a one-size-fits-all solution. Monitoring, cost, and side-effects must be weighed.
Do children outgrow hypothalamic obesity?
Rarely, early intervention helps
Without early treatment, the condition tends to persist into adulthood. However, lifestyle coaching combined with medical therapy can mitigate the long-term impact.
What's the impact on life expectancy?
Higher risk of secondary disease
Uncontrolled weight gain raises the odds of type-2 diabetes, hypertension, and heart disease, which can shorten lifespan. Early, proactive management flips that trajectory.
Real Stories & Practical Tips
Case study: Adult onset
John's journey after craniopharyngioma
John, 45, underwent surgery for a craniopharyngioma at 38. Within months he packed on 30lb despite sticking to his usual diet. A referral to an endocrinologist revealed hypothalamic obesity. With setmelanotide, structured meals, and weekly CBT, he has now lost 15lb and feels his energy returning.
Case study: Pediatric experience
Lila's school-day challenges
Lila, 9, was diagnosed after her pediatric oncologist noted rapid weight gain post-tumor removal. Her parents started a food-log app to track cravings, introduced short, fun movement breaks at school, and joined a local support group. Over a year, Lila's BMI percentile stabilized, and she regained confidence in the playground.
Top 5 practical hacks
Everyday tools that help
- Use a phone app that sends "time-to-move" alerts every hour.
- Pre-portion snacks into zip-top bags to avoid mindless munching.
- Schedule micro-walks (23 minutes) during TV commercials.
- Swap sugary drinks for flavored sparkling watersame sip, fewer calories.
- Keep a consistent sleep schedule; poor sleep spikes ghrelin, the hunger hormone.
Resources & support networks
Where to find help
Organizations like the and the host expert guides and patient forums. The Rare Diseases Organization also maintains a dedicated hypothalamic obesity page, and there's a lively Facebook support group where families share recipes and encouragement.
Bottom Line
In a nutshell, the main hypothalamic obesity symptomsrapid weight gain, relentless hunger, low metabolism, mood swings, and reduced activityare signals that the brain's energy-balance hub needs help. Recognizing these clues early, securing a multidisciplinary medical team, and embracing a blend of targeted medication, tailored diet, and behavioral strategies can turn a daunting diagnosis into a manageable part of life.
If any of these signs feel familiar, don't wait: schedule an appointment with an endocrinologist, download the free symptom-checklist, and consider joining a community of people who truly understand the journey. You deserve answers, support, and a path forwardlet's take the first step together.
FAQs
What are the first signs that I might have hypothalamic obesity?
The earliest clues are a rapid, unexplained weight gain (often >5 % of body weight in < 6 months) paired with persistent, intense hunger (hyperphagia) that doesn’t improve with usual diet changes.
How do doctors confirm a diagnosis of hypothalamic obesity?
Diagnosis combines a detailed weight‑gain history, hormonal labs (leptin, insulin, cortisol), and an MRI of the hypothalamic region to spot scar tissue, residual tumor or other structural damage.
Can I control hypothalamic obesity with diet and exercise alone?
Because the hypothalamus mis‑reads fullness signals and lowers basal metabolic rate, conventional dieting often fails. Structured meals, NEAT tricks, and low‑glycemic foods help, but most patients need medication or therapy for meaningful results.
What medication options are available for hypothalamic obesity?
Approved options include the MC4‑R agonist setmelanotide, GLP‑1 agonists (e.g., liraglutide) to curb appetite, and off‑label appetite suppressants. Metformin may improve insulin sensitivity. All require specialist monitoring.
Is hypothalamic obesity curable, or only manageable?
There is currently no cure. However, a combination of targeted drugs, personalized nutrition, behavioral therapy, and, in selected cases, bariatric surgery can bring symptoms under control and improve quality of life.