Quick answer: a simple blood test that checks your TSH, free T4 and free T3 is the fastest way to confirm hyperthyroidism. Your doctor will then match those numbers with how you feel and, if needed, add an ultrasound or a radioactiveiodine scan to pin down the cause and plan treatment.
Thats the whole story in a nutshellno jargon, no endless scrolling. If youre wondering whether those fluttery heartbeats or sudden weight loss mean something more serious, keep reading. Ill walk you through why catching it early matters, what the exact diagnostic criteria are, and what the next steps look like, all in a friendly, downtoearth style.
Why Diagnosis Matters
Risks of Untreated Hyperthyroidism
Leaving hyperthyroidism unchecked is a bit like ignoring a small leak in a dam. At first it seems harmless, but over time the pressure builds. Common complications include:
- Irregular heart rhythms (atrial fibrillation) that can increase stroke risk.
- Bone loss leading to osteoporosisespecially concerning for women over 50.
- Pregnancy issues such as preeclampsia or low birth weight.
- In rare cases, a thyroid storma sudden, lifethreatening surge of hormones.
Benefits of Early Detection
Spotting the condition early swaps those scary whatif scenarios for a clear, manageable plan. Early treatment often means:
- Symptoms settle faster, so you feel like yourself again.
- Medication doses can stay low, reducing sideeffects.
- Less invasive options (like radioactive iodine) become viable.
Think of it as fixing that leak before the whole dam gives way.
RealWorld Example
Take Sarah, a 34yearold graphic designer. She noticed rapid weight loss, a racing heart, and tremors in her hands. A quick TSH test flagged a suppressed level, and a followup free T4 confirmed hyperthyroidism. Thanks to that early diagnosis, she avoided a potential thyroid storm and got back to her art within weeks.
Diagnostic Criteria
BloodTest Basics
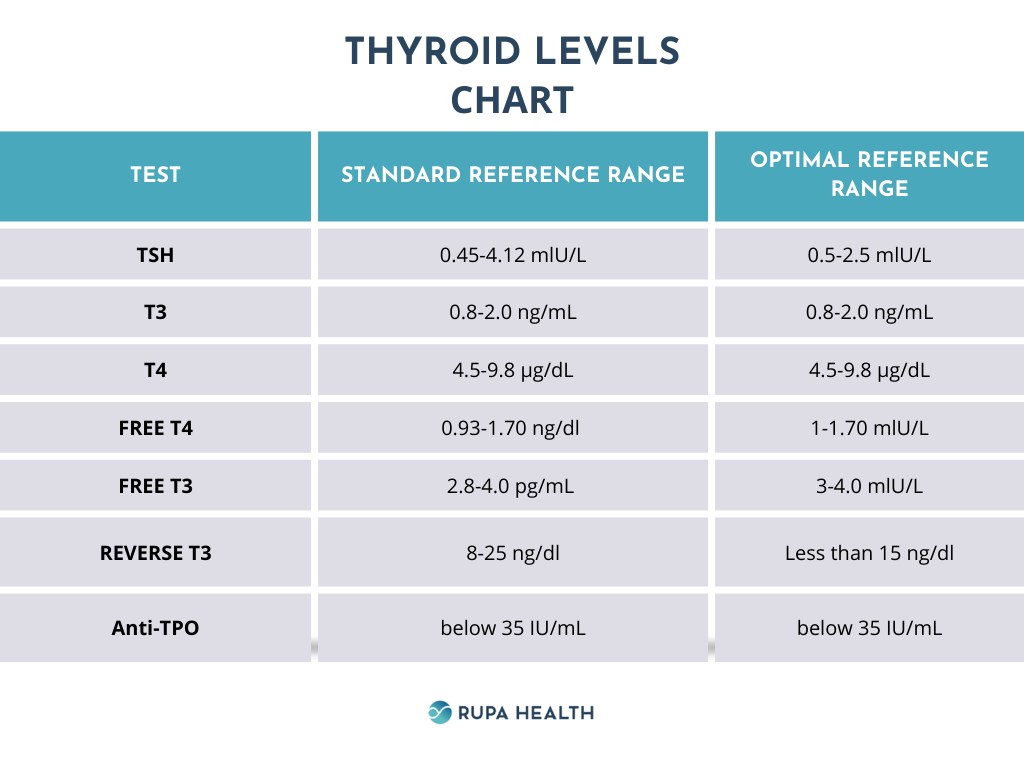
The blood work is the cornerstone. Three numbers give the full picture:
- TSH (ThyroidStimulating Hormone) the most sensitive marker. Low TSH usually means the thyroid is overactive.
- Free T4 the main hormone produced by the thyroid.
- Free T3 the active form that drives most symptoms.
According to the , the combination of a suppressed TSH (<0.4mIU/L) with elevated free T4 or T3 clinches the diagnosis.
What TSH Levels Indicate Hyperthyroidism?
| TSH (mIU/L) | Interpretation |
|---|---|
| <0.4 | Suppressed suggests hyperthyroidism |
| 0.44.0 | Normal usually rules out hyperthyroidism |
| >4.0 | Elevated points toward hypothyroidism |
Additional Labs
Other blood tests help identify the cause:
- Thyroidstimulating immunoglobulin (TSI) or TSHreceptor antibodies high in Graves disease.
- Thyroid peroxidase (TPO) antibodies can appear in autoimmune thyroiditis (still useful for differential diagnosis).
- Calcium and liver enzymes to flag complications or medication sideeffects.
Graves vs. Toxic Nodular Goiter
Graves disease usually shows high antibody levels, whereas a toxic nodular goiter shows normal antibodies but a focal hot spot on scintigraphy. A quick sidebyside table helps keep this straight.
Symptom Checklist
Classic Symptoms
Hyperthyroidism can feel like a speedup button on your body. Common signs include:
- Heat intolerance and sweaty skin.
- Rapid or irregular heartbeat.
- Tremor (especially in the hands).
- Unexplained weight loss despite normal appetite.
- Feeling jittery or anxious.
Hyperthyroidism Symptoms in Females
Women often notice a few extra clues:
- Irregular menstrual cycles or lighter periods.
- Hair thinning, especially around the scalp.
- Increased sensitivity to heat during menopause.
These genderspecific signs can be the missing piece that tips a clinician toward testing.
RedFlag Signs That Need Immediate Care
If you experience any of the following, call your doctor or head to urgent care right away:
- Severe chest pain or shortness of breath.
- Sudden, extreme agitation or confusion.
- Very high fever with vomiting possible thyroid storm.
Imaging Tests
Radioactive Iodine Uptake (RAIU)
The RAIU test measures how much iodine the thyroid absorbs. A high uptake suggests the gland is overactive on its own (like Graves), while a low uptake often points to thyroiditis.
Thyroid Ultrasound
Ultrasound is painless and shows the glands size, texture, and any nodules that might be causing autonomous hormone production. If nodules are suspected, imaging helps guide treatment decisions and distinguishes nodular causes from diffuse disease.
Scintigraphy (I123 or Tc99m)
This scan creates a heatmap of activity. Hot spots indicate overproducing tissue, whereas cold spots often signal nonfunctioning nodules.
Sample Scan Report WalkThrough
The 24hour uptake is 45% (normal 1030%). There are two focal areas of increased activity in the right lobe, consistent with toxic nodular goiter. Decoding that sentence tells you exactly what the doctor is looking atno mystery.
Diagnostic Workflow
StepbyStep Flowchart
- Patient reports symptoms and medical history.
- Firstline labs: TSH if <0.4mIU/L, measure free T4 and T3.
- Confirm hyperthyroidism with elevated free T4 or T3.
- Order antibodies (TSI, TPO) to differentiate cause.
- If antibodies are negative or nodules are suspected, add ultrasound or scintigraphy.
- Refer to an endocrinologist for complex cases or when definitive treatment (radioactive iodine or surgery) is considered.
Decision Points
- Low TSH + high antibodies: likely Graves discuss antithyroid meds.
- Low TSH + normal antibodies + nodules: consider toxic nodular goiter imaging guides whether radioactive iodine or surgery is best.
- Persistent low TSH after treatment: reevaluate dosage or check for medication adherence.
Next Steps After Diagnosis
Discuss Treatment Options
Once the diagnosis is clear, youll explore pathways. The three main roads are:
- Antithyroid drugs (methimazole or propylthiouracil) firstline for most adults.
- Betablockers control rapid heartbeats and tremor while you wait for the antithyroid meds to kick in.
- Definitive therapy radioactive iodine or surgical removal, usually reserved for refractory cases or patient preference.
Lifestyle Tweaks & Hyperthyroidism Diet
Medication works best when you give it a friendly environment. Here are a few easy adjustments:
- Limit iodinerich foods (e.g., kelp, seaweed) if youre heading toward radioactive iodine therapy.
- Eat calciumrich foods (dairy, leafy greens) and VitaminD to protect bone health.
- Stay hydrated, and aim for balanced meals that keep blood sugar steadythis can lessen jitteriness. For people watching diet and blood sugar, small, regular meals and fiber can help manage symptoms while you treat the thyroid issue similar principles to monitoring how strawberries blood sugar respond in sensitive individuals.
Monitoring Schedule
Regular followups are vital. Most doctors recommend:
- Repeat TSH, free T4, and free T3 after 46 weeks of starting antithyroid medication.
- Every 36 months once stable, then annually if youve switched to radioactive iodine.
- Any new symptoms (especially heartrelated) should prompt an immediate lab check.
Conclusion
Getting a clear hyperthyroidism diagnosis is all about a simple blood test, smart followup labs, and, when needed, targeted imaging. Early detection spares you from serious complications, helps you choose the right treatment, and lets you get back to feeling like yourself sooner. If any of the signs we discussed sound familiar, dont waittalk to your doctor and get that test done. Your thyroid health is worth the conversation.
Got questions or personal experiences to share? Drop a comment below. Lets keep the conversation going and help each other stay informed.
FAQs
What blood tests are required for a hyperthyroidism diagnosis?
The core labs are TSH (thyroid‑stimulating hormone), free T4, and free T3. A suppressed TSH combined with an elevated free T4 or T3 confirms hyperthyroidism.
How low must TSH be to indicate hyperthyroidism?
TSH values below 0.4 mIU/L are generally considered suppressed and suggest an over‑active thyroid when paired with high free hormone levels.
When is imaging, such as ultrasound or radioactive iodine uptake, needed?
Imaging is ordered if antibody tests are negative, if nodules are suspected, or when planning definitive therapy (radioactive iodine or surgery).
What antibodies help differentiate the cause of hyperthyroidism?
High thyroid‑stimulating immunoglobulin (TSI) or TSH‑receptor antibodies point to Graves’ disease, while normal antibodies with nodules suggest toxic nodular goiter.
How often should thyroid labs be repeated after starting treatment?
Typically labs are re‑checked 4–6 weeks after initiating antithyroid medication, then every 3–6 months once stable, and annually after definitive therapy.