What if that nagging joint pain isn't just a bad night's sleep? In the next few minutes you'll learn exactly how doctors pinpoint arthritis and what tests you can expect no medical jargon, just clear steps you can follow today.
From a quick blood draw to a simple hand check, we'll walk through every part of the diagnostic journey, so you can feel confident about the results and the treatment options that follow.
Why Accurate Diagnosis Matters
What are the risks of misdiagnosing arthritis?
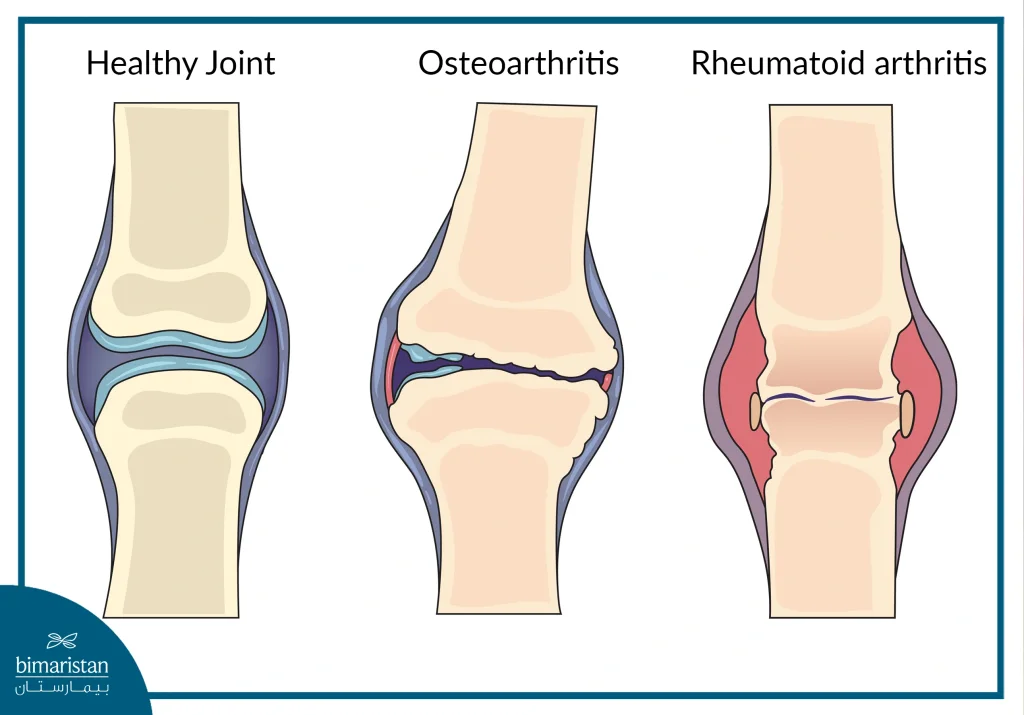
Getting the label wrong can feel like stepping into a maze without a map. If osteoarthritis is mistaken for rheumatoid arthritis, you might miss out on disease-modifying drugs that could slow joint damage. Conversely, treating a harmless sprain as chronic arthritis can lead to unnecessary medication side effects and anxiety.
How does early diagnosis improve outcomes?
Think of arthritis like a small leak in a roof. Spot it early, and a plumber can fix it before the ceiling collapses. Catching rheumatoid arthritis (RA) at the first signs of morning stiffness often means you can start DMARDs (disease-modifying antirheumatic drugs) before irreversible erosion sets in.
Real-world glimpse
Sarah, 45, ignored her hand swelling for months. By the time she saw a rheumatologist, X-rays showed joint erosion. Mark, 52, went in at the first sign of knee stiffness and, with early treatment, started therapy that kept his joints supple for years.
Seven Types of Arthritis
What are the 7 types of arthritis?
- Osteoarthritis (OA) wear-and-tear
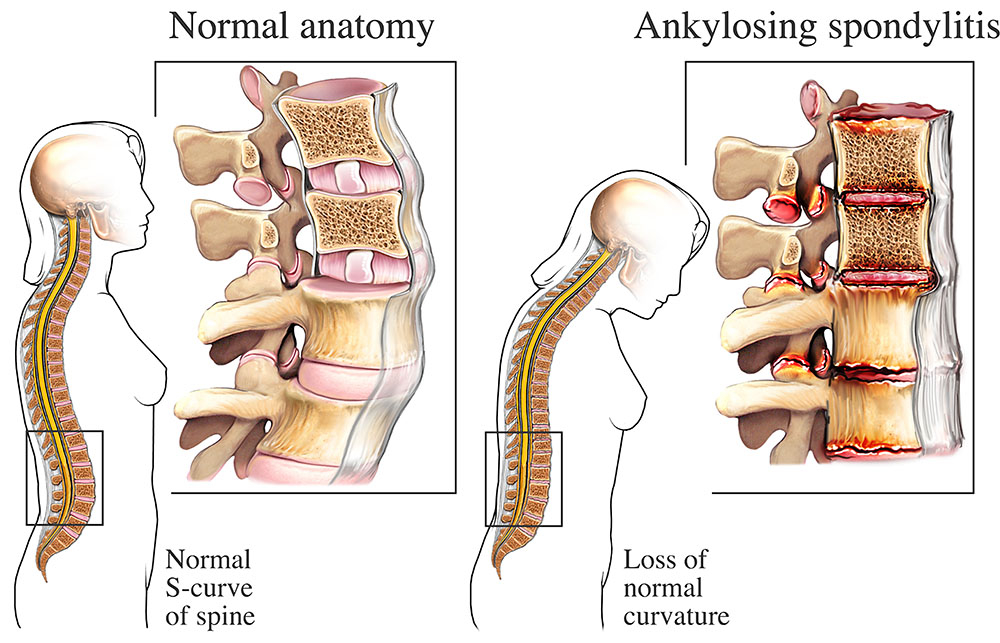
- Ankylosing spondylitis criteria spine-focused
- Rheumatoid arthritis (RA) autoimmune
- Psoriatic arthritis (PsA) linked to psoriasis
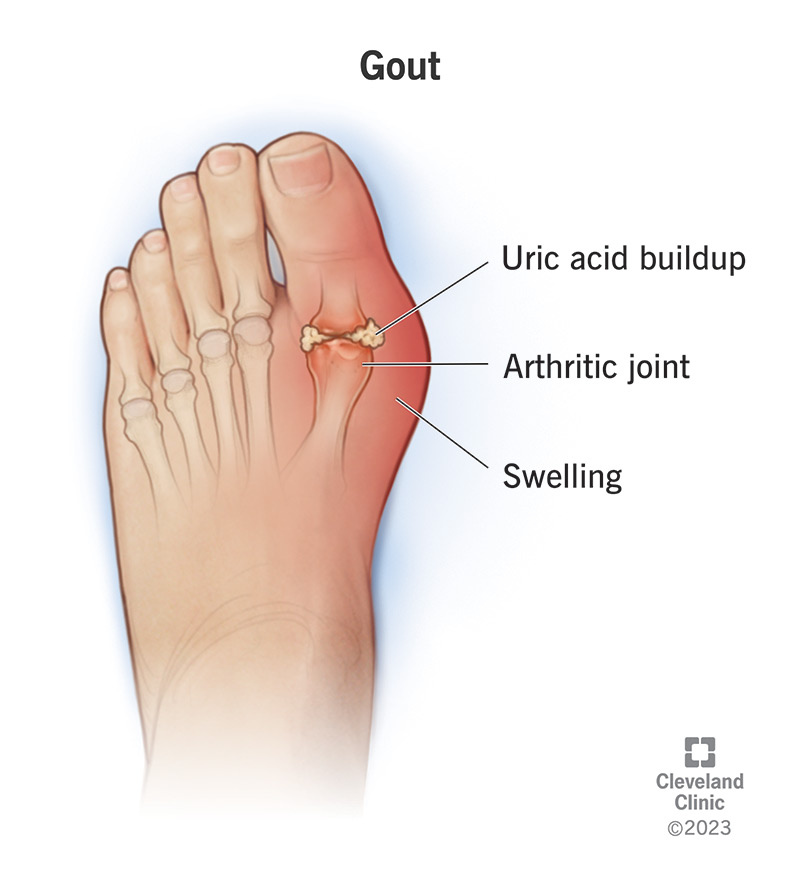
- Gout uric acid crystals
- Juvenile idiopathic arthritis (JIA) childhood onset
- Septic arthritis infection-driven
Which types need special testing?
RA often warrants anti-CCP and rheumatoid factor labs; gout calls for a uric-acid blood test; ankylosing spondylitis leans on HLAB27 genetic screening. Knowing the type helps the doctor choose the right blood tests for arthritis.
Expert insight
Dr. Lina Torres, a board-certified rheumatologist at Mayo Clinic, says, Differentiating OA from early RA is the most common diagnostic challenge in primary care. Her experience underscores why a thorough history matters.
Diagnostic Process Steps
| Step | What Happens | Typical Keywords |
|---|---|---|
| 1 | Medical history review pain pattern, family history, lifestyle | diagnosing arthritis, arthritis symptoms |
| 2 | Physical exam swelling, redness, warmth, range of motion | how to test for arthritis in hands, how to test for arthritis in knees |
| 3 | Laboratory tests (blood work) | blood tests for arthritis |
| 4 | Imaging studies X-ray, ultrasound, MRI | imaging for arthritis, rheumatoid arthritis diagnosis test |
| 5 | Specialized assessments joint aspiration, advanced imaging | early rheumatoid arthritis detection |
| 6 | Referral to a rheumatologist if needed | expert arthritis diagnosis |
How do doctors decide which tests to order?
They start with what hurts you most. A stiff morning hand points to RA; a sharp knee pop after a run suggests OA. Labs follow the clues: elevated ESR or CRP hints at inflammation; high uric acid flags gout.
Visual aid suggestion
Imagine a flowchart: Symptoms Physical Exam Labs Imaging Specialist Referral. That roadmap keeps both patient and doctor on the same page.
Blood Tests Overview
Common blood panels
A CBC checks for infection, while ESR (erythrocyte sedimentation rate) and CRP (C-reactive protein) gauge overall inflammation. They're the first line in many clinics.
Autoantibody tests
Rheumatoid factor (RF) has been around for decades, but anti-CCP (cyclic citrullinated peptide) is more specific for early RA. A positive anti-CCP can mean you're on the fast-track to joint damage if left untreated.
Metabolic tests
Uric acid levels catch gout; Lyme titers rule out infection-related arthritis in endemic areas.
Interpretation tip
If your anti-CCP is high but you only have mild hand pain, don't panic. It's a green flag for your doctor to monitor closely and possibly start a low-dose DMARD.
Credible source
According to the National Institute of Arthritis and Musculoskeletal and Skin Diseases, these labs together improve diagnostic accuracy by up to 80%.
Imaging Options Explained
X-ray basics
Doctors look for joint-space narrowing, osteophytes (bone spurs), and erosions. Hand X-rays can reveal early RA changes that aren't yet visible to the naked eye.
When to use ultrasound vs. MRI
Ultrasound catches synovial fluid and early inflammation in real timegreat for small joints. MRI shines when you need a deep look at cartilage, bone marrow, or the knee's meniscus.
Hand-X-ray protocol & Knee MRI grading
For hands, a standard posteroanterior view is used; for knees, the OARSI (Osteoarthritis Research Society International) grading system guides MRI interpretation.
Comparison table
| Modality | Cost | Availability | Diagnostic Yield |
|---|---|---|---|
| X-ray | Low | Widely available | Good for bone changes |
| Ultrasound | Moderate | Limited to specialists | Excellent for soft-tissue inflammation |
| MRI | High | Specialized centers | Best for early cartilage & bone marrow lesions |
Detect Early Rheumatoid
Early clinical signs
Morning stiffness that lasts longer than 30 minutes, symmetrical swelling of the small joints (like the knuckles), and fatigue that feels out of proportion to the pain.
Key lab markers & imaging clues
Positive anti-CCP, elevated CRP, and erosions on hand X-ray are the trifecta that says RA is on the move.
Real-world example
Emily, 29, woke up with swollen fingers that wouldn't loosen. After a quick anti-CCP test and a hand X-ray, her rheumatologist started her on methotrexate within weeks. Six months later she reported back to normal activities and was hopeful with the ankylosing spondylitis remission approach her care team recommended.
Arthritis Self-Check Quiz
5-question quick quiz
- Do you experience joint pain that worsens with activity? (Yes/No)
- Is morning stiffness longer than 30 minutes? (Yes/No)
- Do you notice swelling, redness, or warmth around joints? (Yes/No)
- Have you lost weight unintentionally? (Yes/No)
- Is there a family history of autoimmune disease? (Yes/No)
What the results mean
- Low risk: Monitor symptoms, stay active, and revisit if things change.
- Medium risk: Schedule a primary-care visit for labs and a basic exam.
- High risk: Ask for a referral to a rheumatologist ASAP.
Disclaimer
This quiz is for educational purposes only and does not replace professional medical advice.
Results and Next Steps
How doctors combine everything into a final diagnosis
Think of it like assembling a puzzle. Each piecehistory, physical exam, lab values, imagingfits together. If most pieces point to RA, the diagnosis is set. If they're mixed, doctors may label it undifferentiated arthritis and watch closely.
When uncertainty remains
Sometimes the picture isn't crystal clear. In those cases, doctors might repeat labs in 36 months, order a follow-up MRI, or simply keep a symptom diary.
Patient checklist for the next appointment
- Copy of all blood test results
- List of current medications (including over-the-counter)
- Symptom diary (pain level, time of day, activities)
- Any family-history notes
Benefits vs Risks
Benefits of a proper diagnosis
Targeted treatment that can halt disease progression, tailored exercise plans such as osteoporosis exercises, and peace of mind knowing you're on the right track.
Potential risks
Overtesting can lead to unnecessary radiation exposure or anxiety from false-positive results. That's why a balanced, shared-decision approach is essential.
Expert voice
Dr. Michael Lee of Johns Hopkins writes, Patients who feel involved in the diagnostic conversation report higher satisfaction and better adherence to treatment plans.
Treatment Options Overview
First-line medications per arthritis type
- Osteoarthritis: NSAIDs (e.g., ibuprofen), topical analgesics, joint-preserving supplements.
- Rheumatoid arthritis: DMARDs such as methotrexate, biologics (TNF inhibitors), and low-dose steroids for flares.
- Psoriatic arthritis: NSAIDs, DMARDs, and newer IL-17 inhibitors.
Nonpharmacologic therapies
Physical therapy, low-impact cardio (like swimming), weight management, and joint-protective splints can all boost outcomes.
Most effective medication for arthritis?
There's no one-size-fits-all answer. For RA, methotrexate remains the gold standard, but biologics can be most effective for patients who don't respond. For OA, the combination of NSAIDs + exercise often yields the best functional improvement.
Conclusion
Accurately diagnosing arthritis starts with listening to your body, getting the right labs, and using imaging wisely. While early detection can dramatically improve outcomes, it's equally important to avoid overtesting and the stress that comes with it. Use the self-check quiz, keep a symptom diary, and don't hesitate to bring your questions to a trusted rheumatologist. The sooner you know what's going on, the sooner you can take charge of your joint health and live the active life you deserve.
FAQs
What initial questions do doctors ask when diagnosing arthritis?
They inquire about pain pattern, duration of morning stiffness, swelling, family history, recent injuries, and any systemic symptoms like fatigue or weight loss.
Which blood tests are most helpful for identifying rheumatoid arthritis?
Rheumatoid factor (RF) and anti‑CCP antibodies are key; elevated ESR or CRP also indicate active inflammation.
When is imaging required during the arthritis diagnostic process?
Imaging is ordered if physical exam or labs suggest joint damage—X‑rays for bone changes, ultrasound for early soft‑tissue inflammation, and MRI for detailed cartilage or bone‑marrow assessment.
How does a doctor decide between osteoarthritis and early rheumatoid arthritis?
They compare symptom symmetry, joint involvement (small vs. weight‑bearing joints), lab results (RF/anti‑CCP), and imaging findings such as erosions (RA) versus osteophytes (OA).
What should I bring to my appointment if I suspect I have arthritis?
Prepare a list of current medications, recent blood test results, a symptom diary noting pain intensity and timing, and any relevant family‑history information.