In the next few minutes youll get the full roadmap: a quick redflag checklist, the basic labs you really need, when imaging becomes mandatory, and a handy differentialdiagnosis table. No fluff, just the answers that matter so you can decide whether to treat, monitor, or refer. If youre also managing coexisting conditions such as restless legs or ADHD, consider how treatments overlap (see resources on restless legs ADHD) to avoid medication conflicts.
Why Structured Algorithm
Problems Without a Plan
When we tackle headaches without a clear framework, we often miss crucial clues or overorder tests. Unstructured approaches can lead to delayed diagnosesthink of a missed aneurysmor unnecessary costs from blanket imaging. A systematic algorithm keeps us focused on what truly matters.
Benefits vs. Risks
| Benefit | Risk |
|---|---|
| Early detection of lifethreatening causes | Potential overtesting if red flags are ignored |
| Efficient use of resources | Patient anxiety from unnecessary scans |
| Clear communication with specialists | Delayed treatment if algorithm is followed too rigidly |
RealWorld Story
Mrs.L, a 52yearold accountant, complained of a sudden, thunderclap headache that lingered for two days. Her primary clinician dismissed it as migraine, postponed imaging, and only after three days did the headache worsen. A CT scan finally revealed a small subarachnoid hemorrhage, costing her weeks of missed work. A simple redflag checklist would have triggered immediate imaging.
Red Flag Checklist
Classic Warning Signs
These are the stopandthink moments. If any appear, jump to urgent evaluation:
- Sudden onset (worst headache ever) think thunderclap.
- Age over 50 with new headache.
- History of cancer, HIV, or immunosuppression.
- Focal neurologic deficits (weakness, vision loss).
- Trauma or recent head injury.
- Systemic symptoms: fever, weight loss, night sweats.
- New headache with altered mental status.
Immediate Actions
When a red flag pops up, the algorithm says:
- Urgent neuroimaging (CT noncontrast first; MRI if needed).
- Consider lumbar puncture if infection or subarachnoid bleed suspected.
- Refer to neurology or emergency department without delay.
According to in the Journal of Emergency Medicine, patients with redflag features who received immediate imaging had a 30% reduction in diagnostic delay.
Initial Clinical Assessment
History Essentials
Ask yourself (or your patient) these key questions:
- When did the headache start?
- How would you describe the pain (pulsating, pressure, stabbing)?
- What makes it better or worse (lights, foods, activity)?
- Associated symptoms: nausea, photophobia, phonophobia?
- Any recent medication changes or overuse?
- Family history of migraine or vascular disease?
Focused Physical Exam
A concise exam can rule out many secondary causes. Include:
- Vital signs (fever, hypertension).
- General appearance (signs of distress).
- Neurologic screen: cranial nerves, motor strength, sensation, gait.
- Fundoscopic exam for papilledema (indicative of increased intracranial pressure).
When to Use a Headache Diary
If the headache pattern is unclear, suggest a diary for at least two weeks. Record date, time, intensity (010 scale), triggers, and response to medication. This simple tool often reveals hidden patterns, like caffeine withdrawal or menstrual correlation.
Laboratory Workup
Necessary Baseline Labs
For most primarycare settings, the following tests cover the common metabolic and inflammatory causes:
| Test | Why It Matters |
|---|---|
| Complete Blood Count (CBC) | Detect anemia, infection, or leukemia. |
| Erythrocyte Sedimentation Rate (ESR) / CReactive Protein (CRP) | Screen for temporal arteritis or vasculitis. |
| Fasting Glucose | Identify hypoglycemia or diabetesrelated headaches. |
| Thyroid Stimulating Hormone (TSH) | Hypo or hyperthyroidism can mimic migraine. |
Labs for Secondary Causes
If red flags exist or the baseline labs are abnormal, broaden the panel:
- Antinuclear Antibody (ANA) for autoimmune disorders.
- Lumbar puncture analysis (opening pressure, CSF cells, glucose, protein) if meningitis or subarachnoid bleed suspected.
- Serum electrolytes and renal function for medication toxicity.
- Coagulation profile if anticoagulant use is present.
Imaging Guidelines
CT vs. MRI
CT scans are fast and excellent for detecting acute hemorrhage or skull fracturesideal in emergency settings. MRI offers superior detail for softtissue lesions, demyelination, and small tumors but takes longer and costs more.
CostEffectiveness Snapshot
| Scenario | Preferred Modality | Reason |
|---|---|---|
| Acute thunderclap | CT noncontrast | Rapid bleed detection. |
| Suspected tumor, chronic | MRI with contrast | Better tissue characterization. |
| Unclear secondary cause, no red flags | Reserve imaging | Avoid unnecessary radiation. |
The algorithm from the recommends imaging only when redflag criteria are met, saving about 20% of unnecessary scans annually.
Headache Differential Diagnosis
Primary Headaches
These are the benign headaches that arent caused by another disease. The three big players:
- Migraine: Pulsating, unilateral, worsens with activity, accompanied by nausea, photophobia, or phonophobia.
- Tensiontype: Pressing or tightening quality, bilateral, mildtomoderate intensity, no aura.
- Cluster: Severe unilateral pain around the eye, lacrimation, nasal congestion, occurring in bouts.
Secondary Headaches
These stem from an underlying condition and warrant a more thorough workup:
- Sinusitis or dental infection.
- Medicationoveruse headache.
- Intracranial hypertension (often in overweight women).
- Infections: meningitis, encephalitis.
- Vascular: subarachnoid hemorrhage, temporal arteritis.
- Neoplastic: primary brain tumors or metastases.
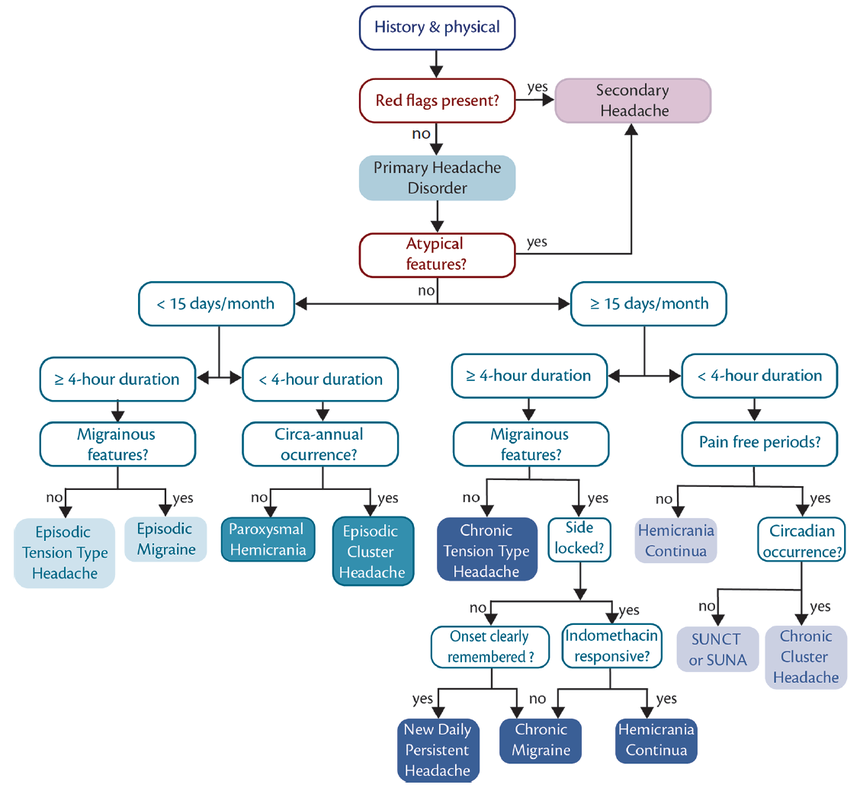
StepbyStep Narrowing
The algorithm starts with redflag screening, then applies the basic labs and imaging decisions. If everything is negative, it moves to the primaryheadache categories, using the IDMigraine criteria (photophobia, nausea, worsening with activity) to confirm migraine, while tensiontype is diagnosed by exclusion.
Management Pathways
Acute Migraine Flow
When you land on a migraine diagnosis, the treatment line looks like this:
- Firstline: NSAIDs (ibuprofen 400600mg) or acetaminophen.
- If inadequate: Triptans (sumatriptan 50100mg) taken early.
- Adjunct: Antiemetics (metoclopramide) for nausea.
- Preventive (if >4 monthly attacks): Betablockers, CGRP monoclonal antibodies, or lifestyle modifications (sleep hygiene, trigger avoidance).
When to Start Preventive Therapy
Consider prevention if any of these apply:
- More than four disabling headaches per month.
- Significant functional impairment (missed work or school).
- Failure of acute treatment after three tries.
AAFP Treatment Highlights
The American Academy of Family Physicians recommends starting with lifestyle changesregular meals, hydration, and stress managementbefore moving to pharmacologic preventives. For patients with contraindications to betablockers, topiramate or amitriptyline are solid alternatives.
Practical Tools & Resources
Downloadable PDFs & PPTs
For quick reference, grab the or the . Both include the flowchart, redflag list, and a concise lab panel.
Interactive Flowchart Apps
Several medical apps (e.g., UpToDate, Medscape) feature builtin headache algorithms that let you swipe through each decision node. Theyre handy for busy clinics where time is precious.
QuickReference Cheat Sheet
Print a onepage cheat sheet: red flags on the left, labs in the middle, imaging thresholds on the right. Keep it on your desk for fast consultation. If your headache is chronic and you suspect an underlying autonomic issue, review common autonomic neuropathy symptoms to spot overlapping signs early.
Case Studies: Experience in Action
Case A Young Adult, New Daily Persistent Headache
Emma, a 28yearold graphic designer, reported a constant, dull headache for three weeks, worsening with screen time. No red flags, normal exam. Labs (CBC, ESR, TSH) were unremarkable. The algorithm guided us to consider medicationoveruse and tensiontype headache. We tapered her ibuprofen, introduced ergonomic breaks, and prescribed lowdose amitriptyline. Within two weeks, her pain score dropped from 7/10 to 2/10.
Case B Elderly Patient, Sudden Onset
Mr.J, 72, woke with a worst ever headache, mild confusion, and leftsided weakness. Redflag checklist triggered immediate CT, revealing a small rightsided subarachnoid hemorrhage. Rapid neurosurgical referral saved his life. The algorithms redflag emphasis proved crucial.
Lessons Learned
Case A shows that even when labs are normal, a structured algorithm helps avoid overtesting and points toward lifestylefocused treatment. Case B illustrates that missing a red flag can be disastrous; vigilance is key.
Putting It All Together
Now you have the complete headache workup algorithm at your fingertips. Start with the redflag checklist, gather a focused history and exam, order the essential labs, decide on imaging only when needed, and then use the differentialdiagnosis table to pinpoint the cause. From there, follow the tailored treatment pathwaywhether its a simple NSAID for tensiontype pain or a comprehensive preventive plan for chronic migraine.
Remember, every headache tells a story. By listening carefully and following a clear algorithm, you turn that story into a diagnosis, a plan, and ultimately, relief.
Conclusion
Using a thoughtful headache workup algorithm bridges the gap between uncertainty and confidence. It protects patients by flagging danger signs early, reduces unnecessary testing, and guides you to the most effective treatmentwhether its a quick pain reliever or a longterm preventive strategy. Download the free PDF and PPT to keep this roadmap handy, and feel free to share your own headache experiences in the comments. Together, we can make every pounding head a little less intimidating.