If youve just been diagnosed with gestational diabetes and youre staring at the newborn, wondering whether your milk will flow enough, youre not alone. Studies show that women with gestational diabetes are up to three times more likely to notice a delayed letdown or feel like theyre not producing enough milk.
The good news? With a few practical tweakstight bloodsugar control, smart pumping habits, and a balanced dietyou can boost your supply and keep breastfeeding safe for both you and baby. Lets dive in together, step by step.
How Diabetes Impacts Milk
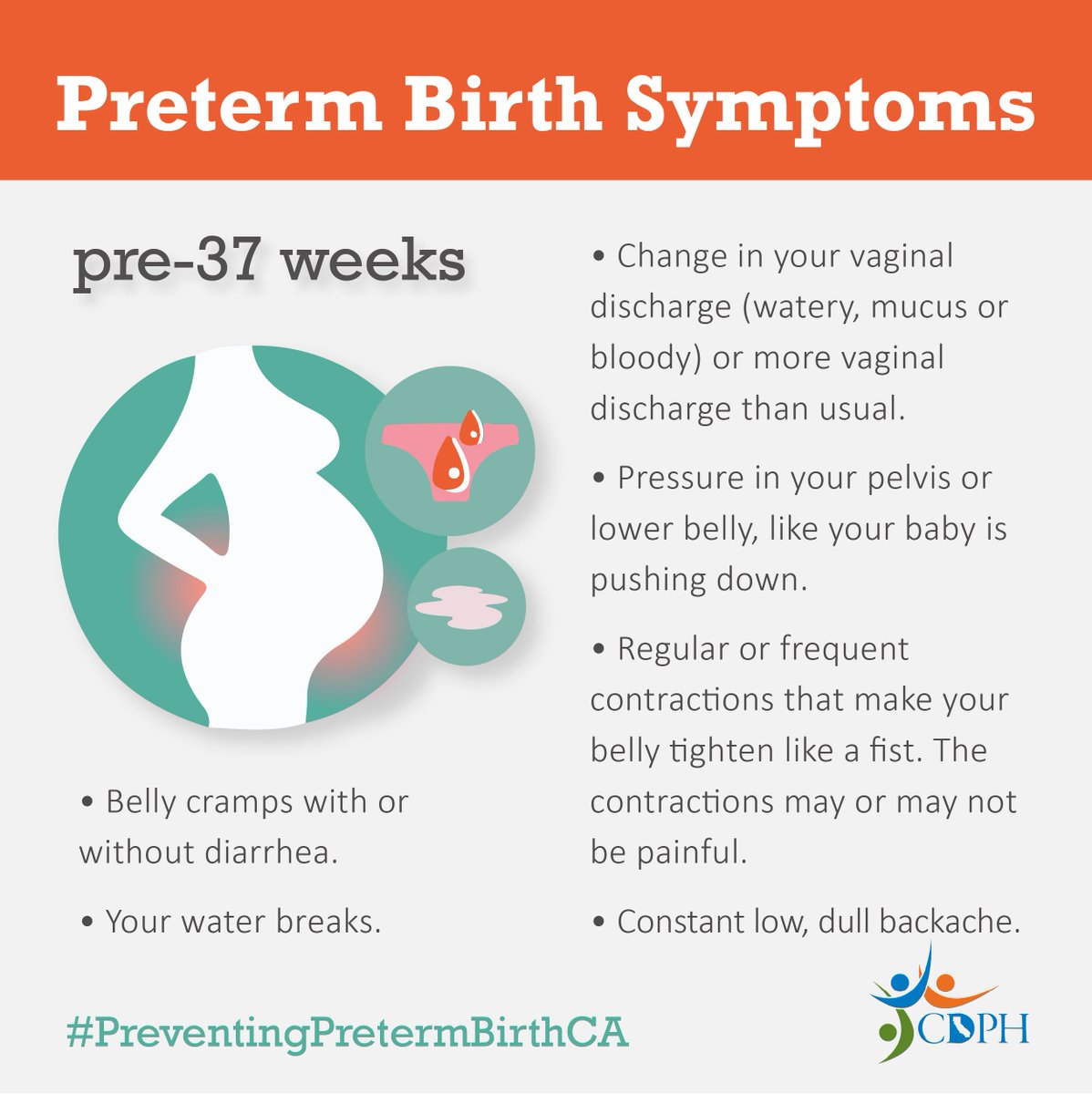
What is delayed secretory activation?
Doctors call the milkcomingin phase lactogenesisII. Normally it happens between 4872hours after birth. When gestational diabetes is in the picture, many moms experience a delay of 48hours or more, meaning the breast stays quiet longer than expected.
Why does diabetes cause low milk supply?
There are three main mechanisms:
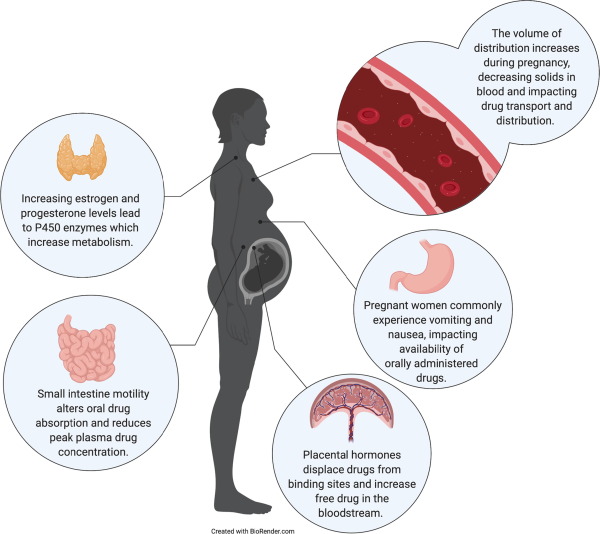
Hormonal imbalance
Insulin resistancecommon in gestational diabetescan blunt prolactin, the hormone that tells your breast to produce milk. When prolactin doesnt get the memo, milk production stalls.
Hyperglycemia and breast tissue
High blood sugar changes how breast cells use glucose for energy. The result? A less efficient milkfactory. A recent found that over 30% of women with gestational diabetes had a noticeable lag in lactogenesisII.
Vascular changes
Diabetes can affect blood flow to the nippleareola complex, making it harder for milk to be pushed out. Think of it like a garden hose with a kinkit still works, but the flow is slower.
Does high blood sugar affect breastmilk composition?
Glucose does cross into breast milk, but the overall protein, fat, and calorie ratios stay largely unchanged. The bigger concern is that spikes in maternal glucose can lead to fluctuating milk volume, not a nutritional deficiency for the baby.
RealWorld Impact Stats
What do the numbers say?
Research comparing moms with and without gestational diabetes shows a clear trend: about 2530% of GDM mothers report perceived insufficient milk versus 1012% of nonGDM moms. The odds ratio for low supply climbs to 2.3 when blood sugar isnt wellcontrolled.
Case study: Janes firstweek journey
Jane (a pseudonym to protect privacy) was diagnosed with dietcontrolled gestational diabetes at 28weeks. She delivered a healthy baby boy, but by day3 she felt the milk wasnt coming in. She blamed the nightshifts at work and the stress of managing her glucose logs.
After a quick chat with her lactation consultant, Jane started frequent pumping (every 2hours, including nighttime) and used a continuous glucose monitor to keep her fasting glucose under 95mg/dL. Within 48hours, her milkcomingin signal fired, and she felt a noticeable rise in output. Janes story is a reminder that even a small tweaklike timing a snack before a pumping sessioncan make a big difference.
Expert voice: Lactation consultants checklist
According to a certified International BoardCertified Lactation Consultant (IBCLC), moms with gestational diabetes should:
- Monitor blood sugar at least four times daily during the first two weeks postpartum.
- Aim for at least 812 milk removal sessions per 24hours.
- Keep a log of pump settings, diaper counts, and glucose readings to spot patterns.
Managing Blood Sugar
What is a diabetic breastfeeding mother diet?
Think of your plate as a steadyenergy engine. Heres a simple 1day example:
- Breakfast: Wholegrain toast, avocado, and a boiled egg (350kcal).
- Snack: Greek yogurt with berries (150kcal).
- Lunch: Grilled chicken salad with mixed greens, quinoa, and oliveoil dressing (450kcal).
- Afternoon snack: Apple slices with almond butter (200kcal).
- Dinner: Baked salmon, sweet potato, and steamed broccoli (500kcal).
Spacing meals every 34hours helps prevent glucose spikes just before you pump or nurse. Hydration is key tooaim for at least 2liters of water daily.
Normal bloodsugar targets while breastfeeding
| Measurement | Target Range |
|---|---|
| Fasting | 7095mg/dL (3.95.3mmol/L) |
| 1hour postmeal | 140mg/dL (7.8mmol/L) |
| 2hour postmeal | 120mg/dL (6.7mmol/L) |
Sticking to these ranges, as recommended by the American Diabetes Association, keeps insulin levels stable, which in turn supports a steady milk flow.
Can untreated diabetes pass through breast milk?
Current research shows that insulinour bodys primary bloodsugar regulatordoes not cross into breast milk in quantities that affect the infant. A comprehensive review in concluded that the risk of a baby developing diabetes from breast milk is negligible. The real focus should be on keeping your own glucose under control.
Boosting Milk Production
Early and frequent milk removal
The simplest, most effective strategy is to treat your breast like a milkbank. Aim for 812 removal sessions in 24hours, including at least one night feeding or pump. Hospitalgrade doubleelectric pumps are great, but a wellchosen handheld pump works fine if youre on a budgetjust make sure the suction feels comfortable.
Power pumping and skintoskin
Power pumping mimics a babys cluster feeding, sending a moremilkplease signal to your glands. Try 10minutes on, 10minutes off, repeating for an hour, twice a day. Pair this with skintoskin time: the warmth and oxytocin surge can shave off a day or two from lactogenesisII, even for moms juggling insulin therapy.
Herbal and medical galactagoguesare they safe?
Fenugreek and blessed thistle are popular milkboosters, but they can also lower blood sugar, which might complicate your diabetes management. If youre considering a supplement, talk to your OBGYN or a diabetes educator first. Prescription options like domperidone have shown promise in clinical trials, but they require a doctors approval and close monitoring.
Rest, hydration, and stress management
It sounds clich, but fatigue and stress raise cortisol, which can blunt prolactin. Here are a few quick selfcare hacks:
- Nap while the baby napsuse a supportive pillow to keep your shoulders relaxed.
- Sip water with a splash of lemon every hour to stay hydrated.
- Try 5minute diaphragmatic breathing before each pumping session; it can trigger oxytocin release.
When to Seek Professional Help
Red flags to watch
If, after a full week, you still feel your supply is low, your baby is losing weight, or your glucose readings keep jumping above 140mg/dL postmeal, its time to call in the cavalry. Persistent low output beyond day7, especially paired with infant lethargy or jaundice, warrants immediate attention.
Who can help?
- Lactation consultant: Provides handson positioning, pump troubleshooting, and customized feeding plans.
- Endocrinologist or diabetes educator: Finetunes insulin dosing or oral meds for the postpartum period.
- OBGYN or midwife: Monitors overall health, especially if youre still on insulin.
- Pediatrician: Ensures the babys growth curve stays on track.
Community resources
Online peer groupslike the Gestational Diabetes Breastfeeding subredditcan be a lifeline. Local chapters of La Leche League often have specialistled sessions for moms with medical conditions. For information on how stress affects gestational diabetes, consider reading about stress gestational diabetes which offers practical stressmanagement tips that can help stabilize blood sugar while you establish breastfeeding.
Balancing Benefits & Risks
Breastfeeding while managing gestational diabetes offers clear perks: it helps regulate maternal blood glucose, reduces the babys future risk of obesity, and builds a unique immune connection. The flip side is the potential for delayed milk onset and the extra mental load of juggling glucose logs and pump schedules.
The key is balance: stay informed, monitor your numbers, and lean on professionals when you need a boost. Remember, every drop you produce is a win, even if the journey feels a bit bumpy.
Conclusion
Gestational diabetes can throw a curveball at your milk supply, but its far from a dead end. By keeping your blood sugar in check, pumping often, and giving yourself grace, you can turn low supply into steady flow. If youre feeling uncertain, reach out to a lactation consultant or diabetes educatortheyre there to help you thrive. Have you tried any of these tricks, or do you have a story to share? Drop a comment below, and lets support each other on this beautiful, messy, milkfilled adventure.
FAQs
How long does lactogenesis II usually take for moms with gestational diabetes?
Normally milk “coming in” occurs 48‑72 hours after birth. With gestational diabetes it can be delayed up to 96 hours, so expect a possible extra day before your milk volume rises.
Can insulin or oral diabetes meds lower my milk production?
Insulin itself does not enter breast milk and does not directly suppress prolactin. However, doses that cause hypoglycemia can reduce feeding frequency, indirectly decreasing supply. Always discuss dose timing with your diabetes educator.
Are there safe galactagogues I can use while managing blood‑sugar levels?
Herbs like fenugreek or blessed thistle may lower glucose, so they should be used only after talking to your provider. Prescription galactagogues such as domperidone are an option, but they require medical supervision.
How many pumping or nursing sessions should I aim for in the first two weeks?
Target 8‑12 milk‑removal sessions every 24 hours, including at least one nighttime feed or pump. This frequent stimulation helps stabilize prolactin and speeds up lactogenesis II.
When is it time to call a lactation professional for low supply?
If after seven days you still notice < 8 wet diapers a day, a baby weight loss > 10 %, or you’re consistently unable to pump ≥ 30 ml per session, contact an IBCLC right away.