Hey there, friend. If youve ever found yourself staring at a pad that seems to soak up the world or wondering why youre spotting on days that feel totally random, youre probably dealing with something called dysfunctional uterine bleeding (often shortened to DUB). In a nutshell, its a hormonal hiccup that makes the lining of your uterus shed at the wrong time or in the wrong amount. Below, well walk through what causes it, how you can tell its happening, how doctors figure it out, andmost importantlywhat you can actually do about it.
What Is DUB?
Definition and medical name
DUB is a type of that isnt caused by a structural problem such as fibroids or polyps. In medical charts youll see it listed under the ICD10 code N92.0, which helps insurers and providers keep track of the diagnosis.
How DUB fits into AUB classification
| Category | Typical Cause | Example |
|---|---|---|
| Dysfunctional Uterine Bleeding (DUB) | Hormonal imbalance, anovulatory cycles | Irregular heavy flow without structural abnormality |
| Structural Abnormal Uterine Bleeding | Fibroids, polyps, adenomyosis | Bleeding linked to a visible growth on ultrasound |
| Coagulopathic Bleeding | Bloodclotting disorders | Bleeding that doesnt stop despite medication |
Why it matters
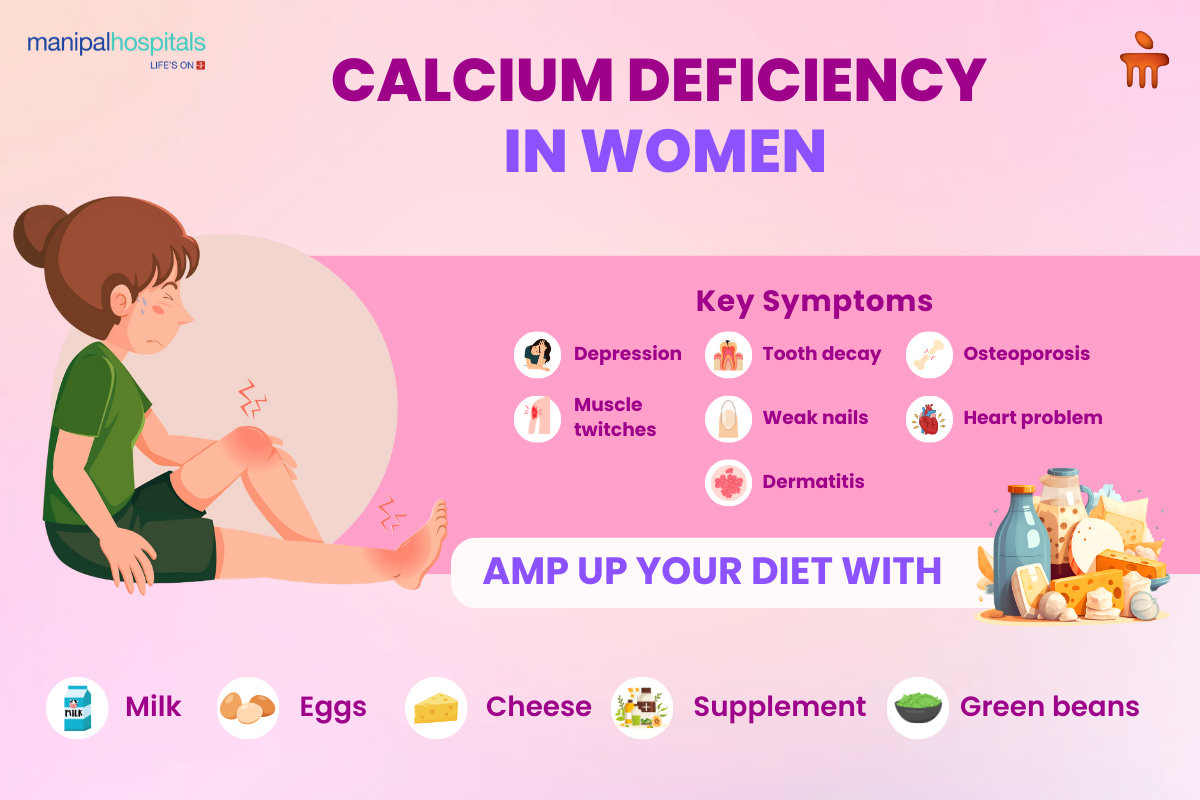
- Chronic heavy bleeding can lead to irondeficiency anemia.
- Unpredictable cycles disrupt daily life and can affect mental wellbeing.
- In some cases, the hormonal environment may influence fertility.
Expert insight
According to Dr. Emily Rivera, MD, a boardcertified OBGYN at the Cleveland Clinic, DUB accounts for roughly a third of all menstrual complaints we see in primary care. Recognizing it early helps prevent unnecessary surgeries.
Common Causes
Hormonal imbalances
Your menstrual cycle is a finely tuned dance between estrogen and progesterone. When that rhythm gets offbeatoften during an anovulatory cycle where the ovary doesnt release an eggthe lining can become overly thick and then slough off all at once, causing a heavy or prolonged bleed.
Medications that trigger DUB
Some drugs mess with your hormones or bloods ability to clot. Common culprits include:
- Combined oral contraceptives (especially when you switch brands)
- Anticoagulants such as warfarin or newer direct oral anticoagulants
- Antidepressants like SSRIs, which can affect serotonin pathways linked to bleeding
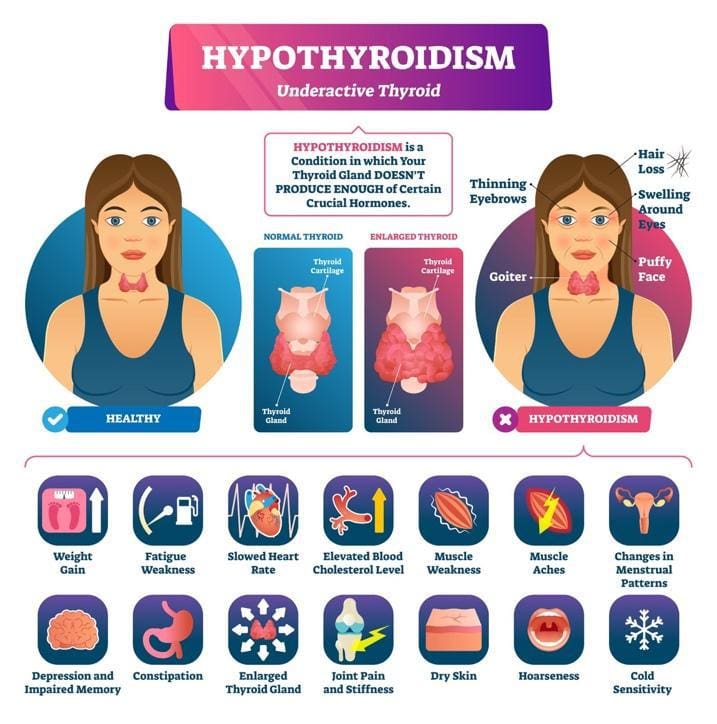
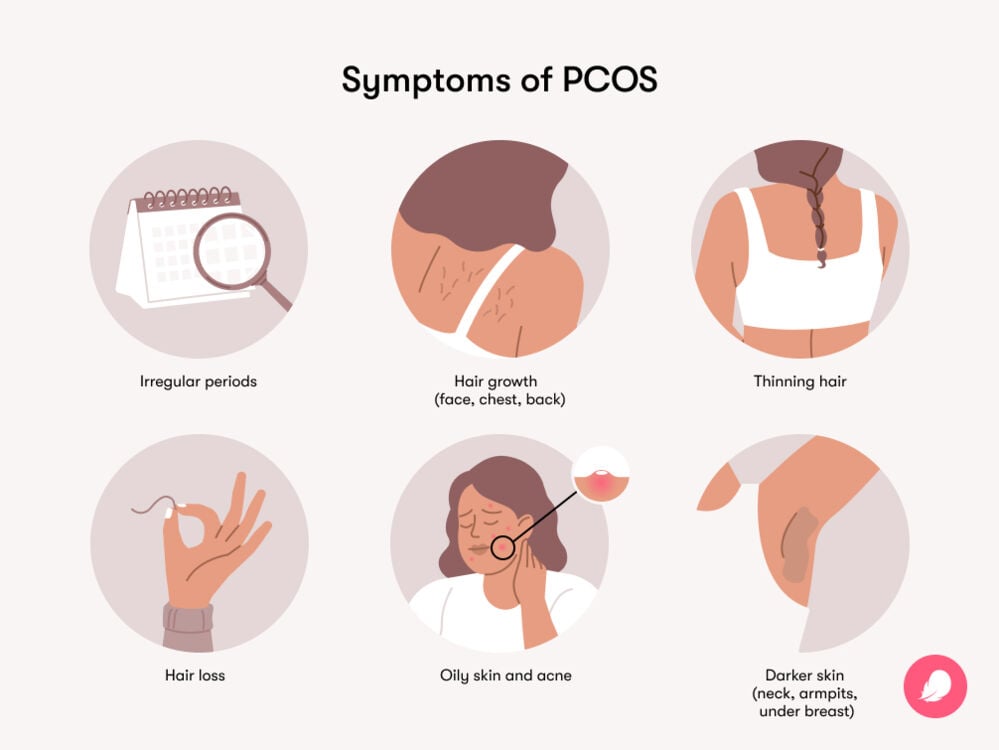
Underlying health conditions
Conditions like polycystic ovary syndrome (PCOS), thyroid disorders, and inherited bleeding disorders (e.g., von Willebrand disease) often show up as DUB on the surface. When you hear a doctor talk about , theyre usually referring to DUB as the symptom. People with lean PCOS may present with irregular or heavy bleeding despite not having classic metabolic signs, so clinicians often consider a broad hormonal workup.
Lifestyle factors
Stress, rapid weight loss or gain, and intense exercise can all tip the hormonal scales. Think of it like a seesawpush too hard on one side, and the balance is lost.
Personal story
Maria, a 28yearold graphic designer, noticed that after starting a new lowcarb diet, her periods became erratic and sometimes lasted two weeks. A simple blood test revealed a mild thyroid deficiency, and once her thyroid was treated, her bleeding patterns returned to normal. Stories like Marias remind us that the body talks, we just need to listen.
Bleeding Symptoms
Typical bleeding patterns
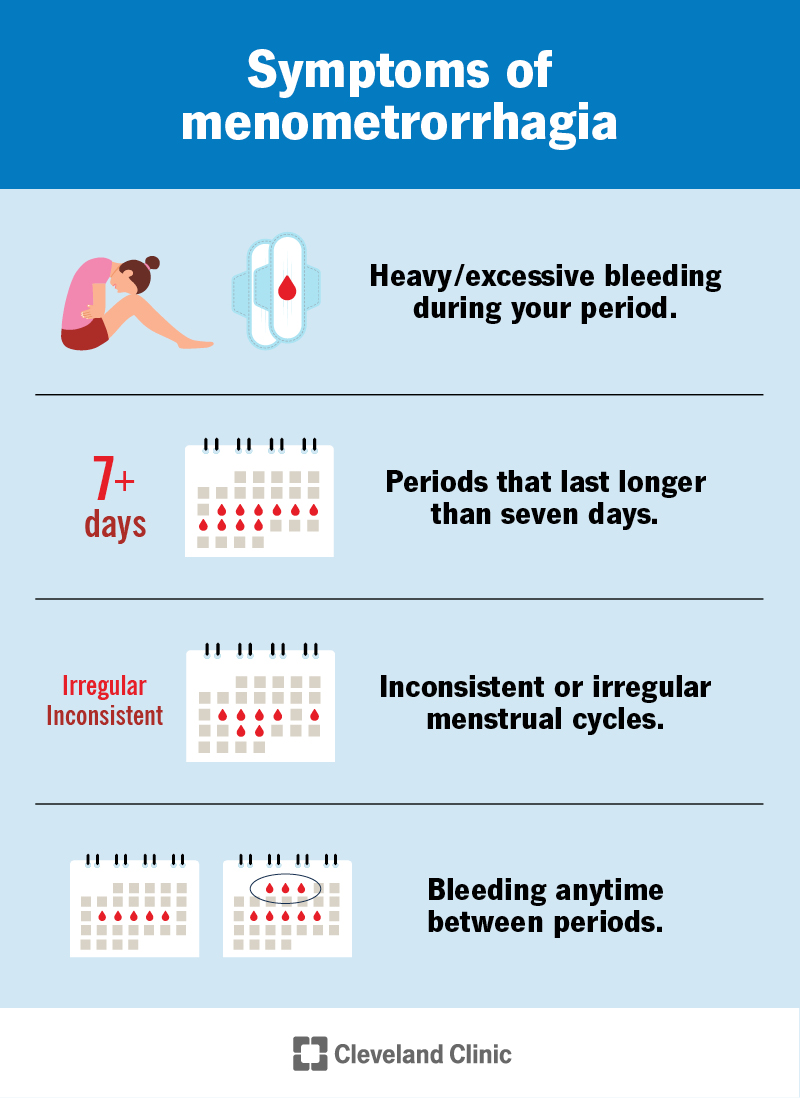
If youre experiencing any of the following, its worth talking to a healthcare provider:
- Spotting between periods that lasts more than a few days.
- Periods that last longer than 7days or require changing a pad every hour.
- Sudden, heavy flow that soaks through a regular pad in under an hour.
When symptoms overlap
| Condition | Key Differences |
|---|---|
| Dysfunctional uterine bleeding | Hormonal cause, no structural lesion on ultrasound |
| Fibroids | Uterus may feel enlarged; ultrasound shows solid masses |
| Endometrial polyps | Localized growth inside uterine cavity, often seen on hysteroscopy |
| Endometrial cancer | Postmenopausal bleeding, usually persistent and accompanied by other risk factors |
Redflag signs
If you notice any of these, seek care right away:
- Sudden drop in energy or shortness of breath (possible anemia).
- Bleeding that soaks through a tampon in less than 30minutes.
- Severe pelvic pain, fever, or foulsmelling discharge.
Case snapshot
Jessica, a 35yearold teacher, logged her cycles in a free phone app for three months. She saw a pattern of 10day bleeds followed by 5day gaps. When she showed the chart to her OBGYN, the doctor ordered a hormone panel, confirming an anovulatory cycleclassic DUB.
How Doctors Diagnose
Medical history & symptom diary
Before any test, your clinician will ask about your menstrual history, medications, stress levels, and any recent weight changes. A simple bleeding lognot more than a pagecan be a gamechanger.
Physical exam & pelvic exam
During a pelvic exam, the doctor checks the size and shape of the uterus, looks for tenderness, and feels for any masses. Most DUB cases have a normallooking uterus, which helps rule out structural causes.
Laboratory tests
- Complete blood count (CBC) to check for anemia.
- Thyroidstimulating hormone (TSH) test.
- Coagulation profile if youre on blood thinners.
- Hormone levels (estradiol, progesterone) when indicated.
Imaging & procedures
Transvaginal ultrasound is the goto method to ensure theres nothing hiding inside. If the ultrasound is clear but bleeding persists, an endometrial biopsy may be performed to rule out hyperplasia or cancer.
Coding note
When documenting, clinicians typically use ICD10 N92.0 for excessive, frequent, and irregular menstruation the technical term for DUB.
Effective Treatment Options
When to watch & wait
If bleeding is mild (less than 80mL per cycle) and youre not anemic, many doctors recommend a watchful waiting approach. Keep a log, maintain a balanced diet, and schedule a followup in 36 months.
Medical therapies
These are the most common dysfunctional uterine bleeding treatment options:
- Combined oral contraceptives (COCs) stabilize hormone swings.
- Progestinonly pills or injectable depot medroxyprogesterone acetate (DMPA) thin the endometrium.
- Levonorgestrelreleasing intrauterine system (LNGIUS, e.g., Mirena) a setandforget device delivering lowdose hormone locally.
- Tranexamic acid an antifibrinolytic that reduces bleeding volume during periods.
- Nonsteroidal antiinflammatory drugs (NSAIDs) help reduce both pain and blood loss.
| Therapy | Pros | Cons |
|---|---|---|
| COCs | Regulates cycle, easy to start | May cause mood changes, not for smokers over 35 |
| Progestinonly | Good for those who cant take estrogen | Irregular spotting for first few months |
| LNGIUS | Longlasting (35years), high efficacy | Insertion discomfort, higher upfront cost |
| Tranexamic acid | Fast relief during heavy days | Only works while youre taking it |
Surgical interventions
When medication isnt enough, doctors may suggest one of the following:
- Endometrial ablation destroys the uterine lining, reducing or stopping periods.
- Hysteroscopic polypectomy removes small growths that could be contributing.
- Hysterectomy removal of the uterus; a lastresort option for severe, refractory cases.
Emerging & alternative options
Some patients find relief with herbal remedies such as chasteberry (Vitex agnuscastus), but evidence is limited. Always discuss with your provider before starting anything new.
Managing sideeffects & risks
Every option has tradeoffs. Hormonal treatments can cause weight gain, mood swings, or spotting; surgical options carry typical procedural risks. The key is an open dialogue with your providerask questions, voice concerns, and together decide what feels right for your body.
Expert tip
According to the American College of Obstetricians and Gynecologists (ACOG), shared decisionmaking improves satisfaction and outcomes for women with abnormal uterine bleeding. In practice, that means your doctor should walk you through the pros and cons, not just hand you a prescription.
Lifestyle & Prevention
Nutrition & weight management
Ironrich foods (spinach, lentils, red meat) help rebuild reserves if youve been anemic. Maintaining a healthy body mass index (BMI) can also keep estrogen levels more stable.
Exercise & stress reduction
Regular moderate activitythink brisk walks, yoga, or swimminghelps regulate hormones. Stressrelief techniques such as meditation or deepbreathing can blunt the HPAaxis spikes that worsen hormonal chaos.
Tracking your cycle
Apps like Clue or Flo let you log flow intensity, duration, and any accompanying symptoms. Most have export features you can bring to your appointment, making the diagnostic talk smoother.
Medication review
Ask your pharmacist or doctor to review any prescription or overthecounter meds youre taking. Even common NSAIDs can affect platelet function, which might amplify bleeding.
Safety checklist
- Is the bleeding soaking through a pad in <1hour?
- Do you feel unusually tired or dizzy?
- Has there been a recent change in weight, stress, or medication?
Helpful Resources
For deeper dives, check out these trusted sources (theyre all reputable medical sites, not just marketing fluff):
Conclusion
Living with dysfunctional uterine bleeding can feel like an endless cycle of uncertainty, but the good news is that its usually manageable. By understanding the hormonal roots, recognizing the warning signs, and working closely with a qualified clinician, you can reclaim a predictable, healthier rhythm. Keep a simple diary, stay on top of your nutrition and stress levels, and dont shy away from asking tough questions during appointments. If youve navigated DUB before, share your story in the commentsyour experience might be the lifeline another reader needs. And if youre just starting to explore this topic, feel free to reach out with any questions; were here to walk this journey together.
FAQs
What causes dysfunctional uterine bleeding?
DUB is usually triggered by hormonal imbalances such as anovulatory cycles, thyroid disorders, polycystic ovary syndrome, stress, rapid weight changes, or certain medications that affect clotting or hormone levels.
How do doctors diagnose dysfunctional uterine bleeding?
Diagnosis starts with a detailed menstrual history and a symptom diary, followed by a pelvic exam, blood tests (CBC, TSH, coagulation profile), and a transvaginal ultrasound to rule out structural problems. An endometrial biopsy may be ordered if bleeding persists.
What are the first‑line medical treatments for DUB?
Common non‑surgical options include combined oral contraceptives, progestin‑only pills or injections, the levonorgestrel‑releasing intrauterine system (Mirena), tranexamic acid for heavy days, and NSAIDs to reduce pain and bleeding.
When should I consider surgical options for DUB?
Surgery is considered when medication fails to control bleeding, when anemia is severe, or when the woman no longer wishes to preserve fertility. Options range from endometrial ablation (minimally invasive) to hysterectomy as a last resort.
Can lifestyle changes help manage dysfunctional uterine bleeding?
Yes. Maintaining a healthy weight, eating iron‑rich foods, regular moderate exercise, stress‑reduction techniques (yoga, meditation), and reviewing all medications with your provider can all improve hormonal balance and reduce bleeding.