Worried about how doctors decide if diabetes is harming your eyes? In the next few minutes well break down the exact grading system they use, why it matters, and what you can do at each stage.
Why Grading Matters
How grading guides treatment decisions
Think of grading like a traffic light for your retina. When a doctor says youre in mild nonproliferative territory, its a green light to keep monitoring and tighten bloodsugar control. Once you hit proliferative diabetic retinopathy, the light turns amber and youll need more aggressive interventions, such as laser therapy or injections.
Risks of misgrading
When an eye exam underestimates the disease, visionthreatening changes can sneak up unnoticed. Overgrading, on the other hand, may lead to unnecessary procedures and anxiety. Studies from the Scottish screening program have shown that accurate classification cuts the risk of missed sightloss by more than 30% ().
Quickcheck list for patients
Ask your eyedoctor these three questions after your exam:
- What stage am I in?
- How often should I be screened?
- What symptoms should I watch for at home?
Standard Classification Systems
Several systems coexist, each built for a slightly different purpose. Below is a handy sidebyside view.
| System | Stages | Key Features | Typical Use | Source |
|---|---|---|---|---|
| ETDRS (Early Treatment Diabetic Retinopathy Study) | 4stages+DME | Standardized photographic fields, quantitative measures | Clinical trials, research benchmarks | |
| AAO (American Academy of Ophthalmology) | 4stages (NPDRPDR) | Clinical exam + imaging, widely taught in U.S. residencies | Routine practice guidelines | |
| Scottish Grading Protocol | R0R4 (retinopathy) / M0M2 (maculopathy) | Featurebased hierarchy, simple to learn | National NHS screening program | |
| AIAssisted Models (e.g., RSGNet) | 4class & 2class output | Deeplearning on fundus images, rapid triage | Emerging teleophthalmology services |
What is ETDRS?
The ETDRS system was born from a landmark clinical trial in the 1980s. Its strength lies in grading each of seven standardized photographic fields, giving a precise score that predicts future vision loss. When you hear diabetic retinopathy grading etdrs, think of a microscopelevel quality check.
What does AAO say about grading?
The AAO simplifies the picture into the classic four stages of diabetic retinopathy. Its the framework most U.S. eye doctors teach to residents, making it easy for patients to understand what each label really means.
How does the Scottish protocol differ?
Scotlands R and Mgrades separate retinal changes from macular edema, allowing a more granular followup plan. Its a good example of how national screening programs can tailor the global standard to local resources.
When to expect AIassisted grading
Artificialintelligence tools are already being piloted in community clinics. While they can flag suspicious eyes in seconds, the final call still rests with a certified ophthalmologistso think of AI as a helpful assistant, not a full replacement.
Four Clinical Stages
Stage1 Mild NonProliferative Diabetic Retinopathy (NPDR)
What youll see on a fundus photo
Microaneurysmstiny red dotsare the sole hallmark. No hemorrhages, no exudates.
Typical symptoms (or none)
Most people feel perfectly fine. Thats why regular screening is a lifesaver.
Recommended followup
Annual retinal exam is usually enough if youre otherwise stable.
Stage2 Moderate NPDR
Key findings
More than 20 microaneurysms, some dotblot hemorrhages, and occasional hard exudates appear.
Why it matters
The fiveyear risk of progressing to severe NPDR jumps to about 15% without intervention.
Management tip
Improve glycemic control, consider early antiVEGF therapy if diabetic macular edema (DME) shows up.
Stage3 Severe NPDR (preProliferative)
421 rule
More than 20 intraretinal hemorrhages in each of the four quadrants, plus venous beading in two or more quadrants, or intraretinal microvascular abnormalities (IRMA) in one quadrant.
Redflag: impending proliferative
At this point the retina is gearing up to grow new, fragile blood vesselswatchful waiting isnt enough.
Treatment options
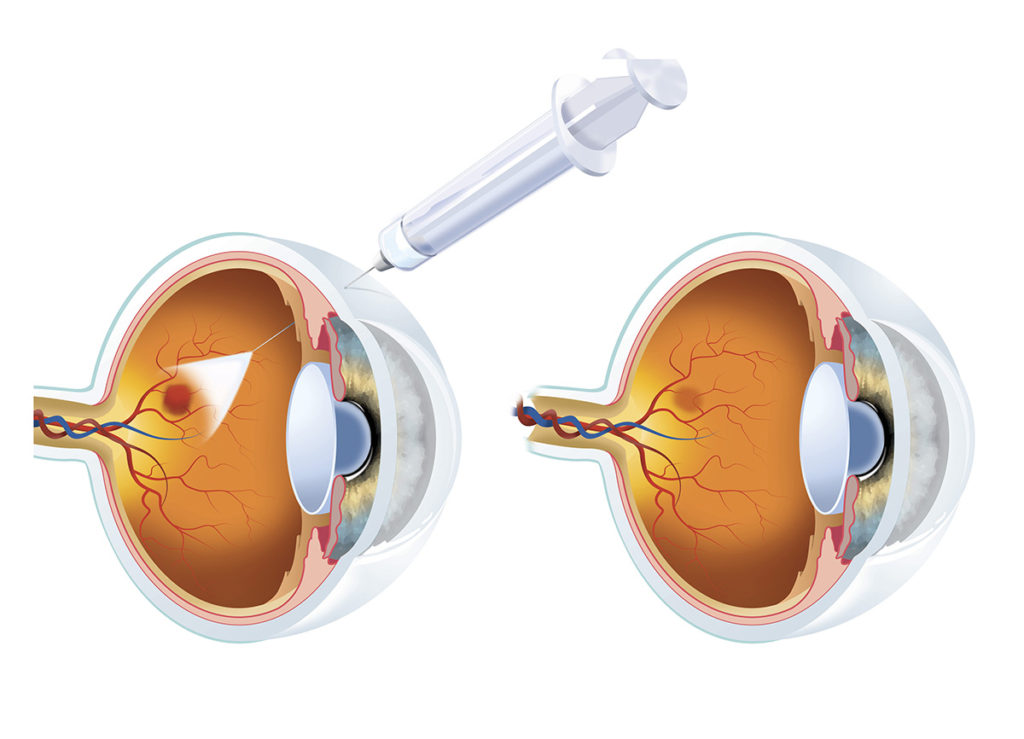
Prompt scatter laser (panretinal photocoagulation) or antiVEGF injections can halt the march to PDR.
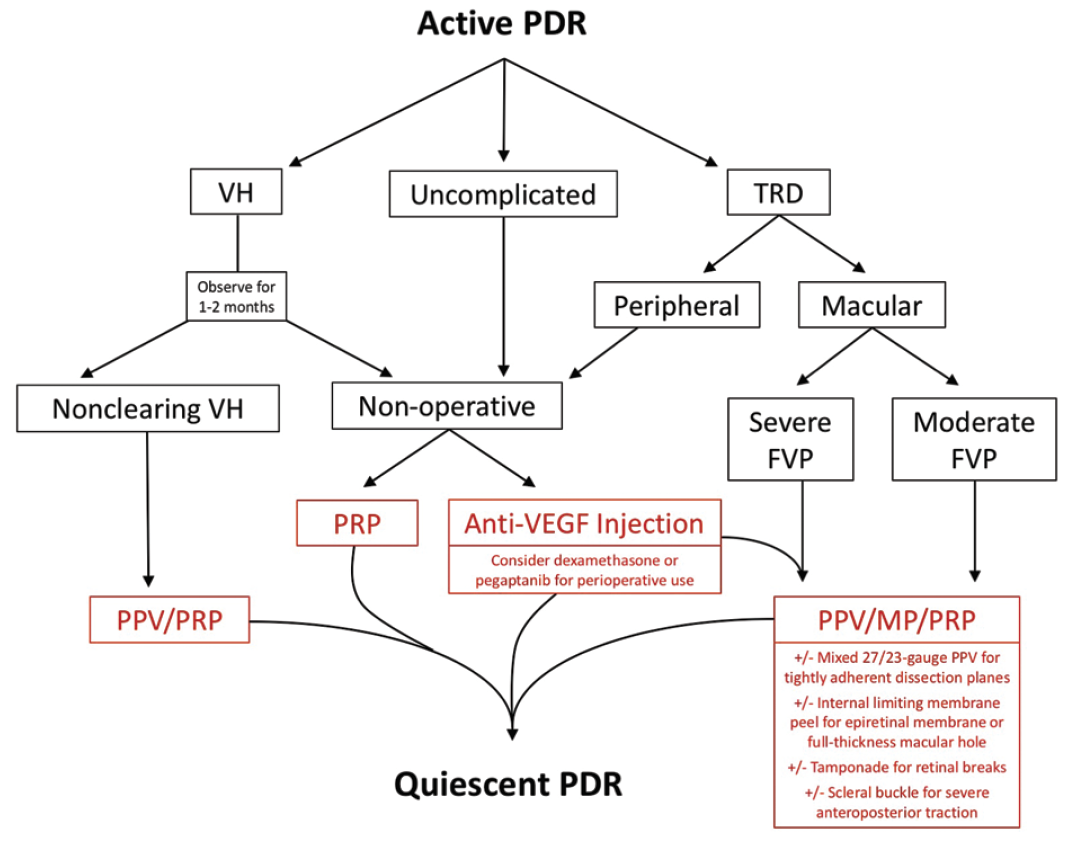
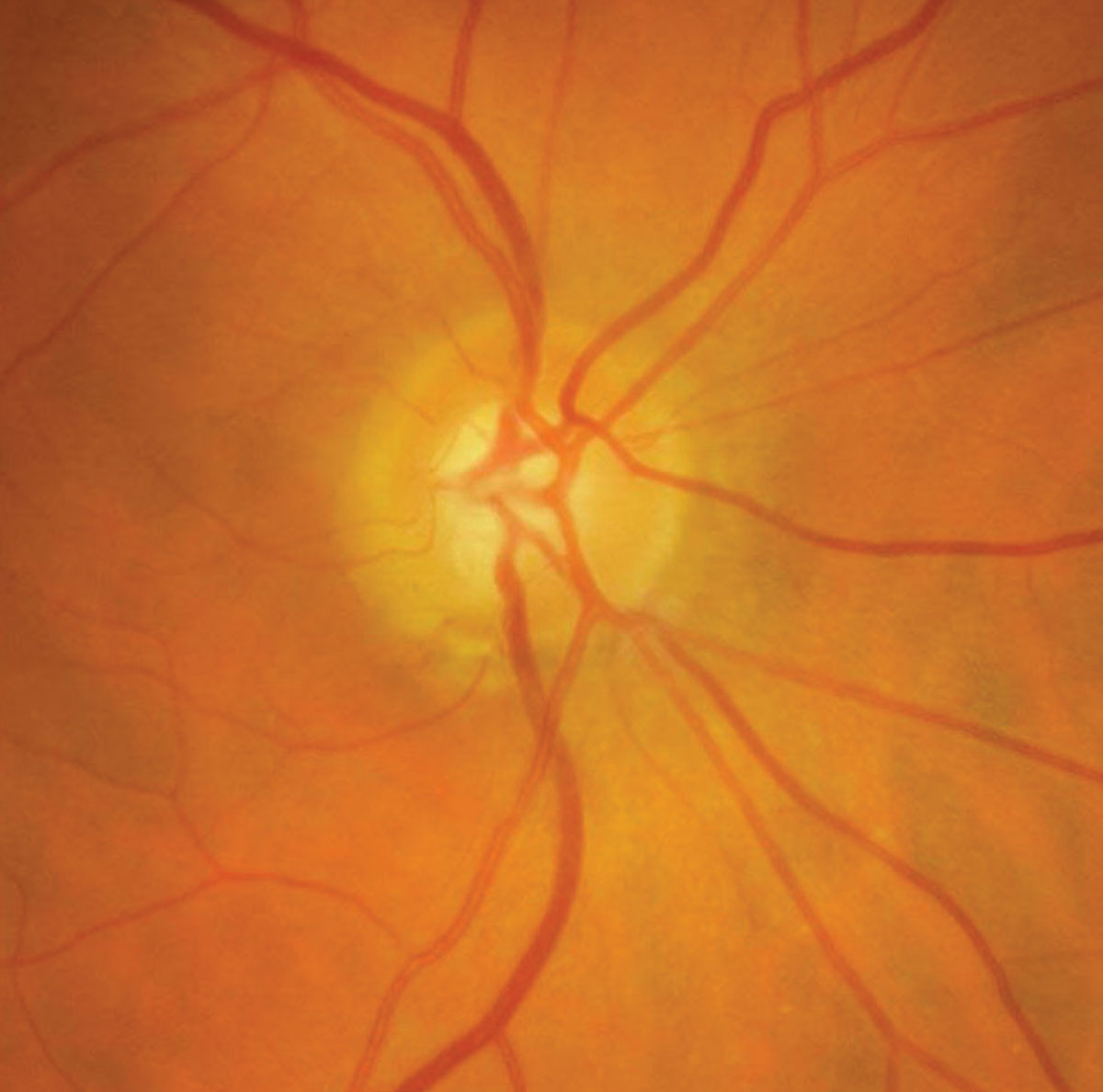
Stage4 Proliferative Diabetic Retinopathy (PDR)
Hallmarks
Neovascularization (new vessels on the optic disc or elsewhere), vitreous hemorrhage, and tractioninduced retinal detachment.
Visionthreatening complications
Bleeding into the vitreous can cause sudden vision loss; scar tissue can pull the retina off the back of the eye.
Standard care
Panretinal laser, vitrectomy for nonresolving hemorrhage, and systemic risk factor control are the cornerstones.
BottomLine Summary for Each Stage
- Mild NPDR: Green lightkeep monitoring.
- Moderate NPDR: Yellow lighttighten control.
- Severe NPDR: Amber lightprepare for intervention.
- PDR: Red lighturgent treatment.
Other Retinal Conditions
Diabetic Macular Edema (DME)
DME gets its own grading because fluid in the macula can impair central vision even when the rest of the retina looks only moderate. The ETDRS also defines DME severity based on retinal thickness measured by OCT.
Hypertensive Retinopathy Grading
High blood pressure can produce cottonwool spots and arteriolar narrowingfindings that sometimes overlap with diabetic changes. While hypertensive retinopathy grading focuses on vessel caliber and exudates, diabetic grading emphasizes microaneurysms and neovascularization. Knowing both helps doctors tease apart mixed causes of vision problems.
Comparison Table
| Feature | Diabetic Retinopathy | Hypertensive Retinopathy | Combined Cases |
|---|---|---|---|
| Primary lesions | Microaneurysms, hemorrhages, neovascularization | Arteriolar narrowing, arteriovenous nicking, cottonwool spots | Both sets may appear; grading must account for each. |
| Common grading scale | 45 stages (including DME) | Grades IIV (KeithWagener) | Separate scores reported, then integrated in management. |
| Treatment focus | Laser, antiVEGF, systemic diabetes control | Bloodpressure meds, lifestyle changes | Dual approachtight BP and glucose control. |
Real World Case Studies
Story #1 Early detection saves sight
Maria, 58, had type2 diabetes for seven years but felt fine. During her routine annual screening, the optometrist spotted a few microaneurysmsstage1 mild NPDR. Because she started stricter glucose monitoring right away, five years later her eyes remain stable, and shes still driving at night without trouble.
Story #2 Missed severe NPDR leads to rapid decline
James, 62, skipped his eye checkup for three years. When he finally went, the retinal images showed severe NPDR plus early neovascular budsessentially an impending proliferative situation. Within six months he developed a vitreous hemorrhage that blurred his vision dramatically. Prompt laser saved his remaining sight, but the episode taught him the cost of neglect.
Expert Insight
Dr. Patel, a retina specialist with the AAO, notes, The moment a patient moves from moderate to severe NPDR, we usually schedule followup every three months. Early detection paired with prompt treatment cuts the risk of blindness by up to 70%.
Bottom Line Actions
Quick Checklist
- Ask your doctor: What stage am I in?
- Confirm how often you need a retinal exam.
- Know the redflag symptoms: new floaters, sudden blurry vision, dark spots.
- Maintain bloodsugar <7% HbA1c and bloodpressure <130/80mmHg.
Lifestyle Tips
Eating a rainbow of vegetables, staying active, and keeping regular appointments are the small habits that add up to big protection for your eyes. Remember, the grading system isnt a judgmentits a roadmap that helps you and your doctor stay one step ahead of the disease.
Conclusion
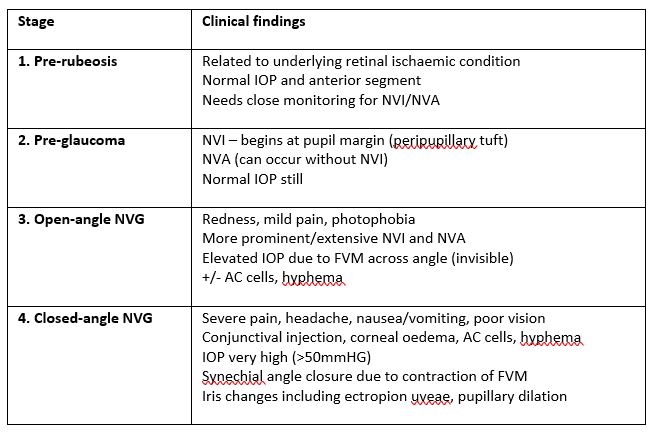
Understanding diabetic retinopathy grading empowers you to catch eye disease early, choose the right treatment, and protect the vision you rely on every day. Whether youre navigating the four classic stages, comparing ETDRS with AAO guidelines, or hearing about the latest AIassisted tools, the key is regular screening and open communication with your eyecare team. Take the checklist, ask those three questions at your next appointment, and share what youve learned with anyone you lovebecause a little knowledge can keep a whole familys sight safe. For patients noticing new eye symptoms related to glaucoma risk factors, consider learning about neovascular glaucoma symptoms as part of your broader eye health awareness.
FAQs
What is diabetic retinopathy grading?
Diabetic retinopathy grading is a system doctors use to classify the severity of eye damage caused by diabetes, guiding treatment and follow-up.
How many stages are there in diabetic retinopathy?
There are four main stages: mild, moderate, severe non-proliferative, and proliferative diabetic retinopathy.
What does mild NPDR mean?
Mild NPDR means early changes like microaneurysms are present, but vision is usually unaffected and monitoring is recommended.
When is treatment needed for diabetic retinopathy?
Treatment is typically needed in proliferative diabetic retinopathy or if diabetic macular edema is present.
What is the difference between NPDR and PDR?
NPDR is non-proliferative, with damaged blood vessels but no new growth; PDR is proliferative, with new, fragile vessels that can bleed.