Got a diagnosis of diabetic autonomic neuropathy and feel overwhelmed? Youre not alone. In a nutshell, treatment centers on three things: tightening your bloodsugar control, using medicines that target the specific symptoms (like low blood pressure or stomach emptying problems), and tweaking daily habits so you feel steadier each day. Below youll find a friendly, stepbystep guide that explains how doctors figure out whats going on, which drugs actually work, and practical tips you can start using right now.
Think of this as a chat over coffee with a friend whos been through the maze and wants to hand you a map. Well talk about the science (in plain language), share realworld stories, and give you tools to weigh benefits against risks. Ready? Lets dive in.
What Is It?
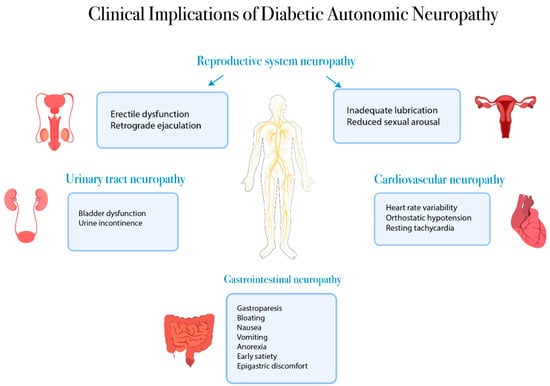
Diabetic autonomic neuropathy (often shortened to DAN) is a type of nerve damage that creeps in when high bloodsugar levels over time start to mess with the autonomic nervous systemthe part of your nervous system that runs in the background, controlling heart rate, digestion, sweating, bladder function, and more. When those nerves get fried, you might notice things like feeling dizzy when you stand up, persistent nausea, or sweaty palms that seem out of place.
Imagine your body as a house with an HVAC system that keeps everything comfortable. Diabetes can rust the thermostat, so the house gets too hot in some rooms and too cold in others. The result? Uncomfortable, unpredictable symptoms that can affect everyday life.
Common early signs include:
- Lightheadedness or fainting when you stand up (orthostatic hypotension)
- Changes in sweatingeither too much or hardly any
- Unexplained constipation or diarrhea
- Sudden heartrate spikes or drops
These symptoms may seem unrelated, but theyre all whispers from the same damaged network of nerves. Recognizing them early can speed up diagnosis and treatment, which is why well talk about in the next section.
How Is Diagnosed?
Diagnosing autonomic neuropathy isnt as simple as a blood test. Doctors combine a detailed symptom history with a few specialized tests that look at how well your autonomic system is working.
Clinical Evaluation
First, your clinician will ask you to describe every odd sensation youve hadno detail is too small. Theyll also check your blood pressure and heart rate while youre lying down and then again after youve stood for a few minutes. A drop of more than 20mmHg in systolic pressure or a heartrate increase of 30bpm signals orthostatic dysfunction.
Specialized Tests
- Heartrate variability (HRV): A simple ECG that measures how your heart rate changes with breathing.
- Tilttable test: You lie on a table that tilts upright while monitors track blood pressure and heart rhythm.
- Gastric emptying study: A scintigraphy scan that watches how quickly food leaves your stomach, essential for spotting gastroparesis.
- Sweat test (Quantitative Sudomotor Axon Reflex Test): Measures how much you sweat in response to a mild stimulus.
Lab work isnt a replacement for these tests, but it helps. Your doctor will look at hemoglobinA1c (to gauge longterm glucose control), electrolytes, and sometimes specific autonomic biomarkers.
FirstLine Treatment Options
Think of firstline treatment as building a strong foundation. Without solid bloodsugar control, any medication you add will have a shaky base to stand on.
Glycemic Control
The Diabetes Control and Complications Trial (DCCT) showed that intensive glucose management can cut the risk of autonomic complications by more than half. That means using insulin or oral agents to keep your A1c as close to target (usually <7%) as possible, while also watching for hypoglycemia.
Medication for Specific Symptoms
| Drug | Primary Target | Typical Dose | Key SideEffects | Evidence Level |
|---|---|---|---|---|
| Midodrine | Orthostatic hypotension | 2.510mg PO TID | Supine hypertension, piloerection | Strong (Mayo Clinic guidelines) |
| Fludrocortisone | Low blood pressure | 0.1mg PO daily | Fluid retention, potassium loss | Moderate (Clinical studies) |
| Metoclopramide | Gastroparesis | 10mg PO QID | Tardive dyskinesia (rare), drowsiness | Strong (UpToDate) |
| Domperidone | Delayed gastric emptying | 10mg PO TID | QT prolongation (monitor ECG) | Moderate (European guidelines) |
| Glycopyrrolate (topical) | Excessive sweating | Apply 24% gel BID | Mouth dryness, blurred vision | Limited (small case series) |
These medicines arent curealls; theyre aimed at making each specific problem less intrusive. Always discuss dosing and monitoring with your endocrinologist or neurologist.
NonDrug Measures
Compression stockings, elevating the head of the bed, and small, frequent meals are lowcost tricks that can dramatically reduce dizziness and nausea. Think of them as the furniture you arrange around the foundationhelpful, inexpensive, and sideeffectfree.
Managing Specific Symptoms
Gastrointestinal Issues
When your stomach decides to take a vacation, even the simplest meals become a battle. Eat smaller portions (about a fistsize), chew thoroughly, and stick to lowfat, lowfiber foods for a few weeks. Adding a prokinetic drug like metoclopramide can jumpstart the movement, while a sprinkle of ginger or peppermint tea can soothe the gut.
Maria, a 58yearold with type2 diabetes, shared that after cutting her meals into six tiny plates and starting metoclopramide, her nausea dropped from daily to once a month. It felt like I got my life back, she told me, laughing.
BloodPressure Swings
Midodrine is the goto for those who feel the world spin when they stand up. Pair it with a simple habit: rise slowly, pause for a few seconds at the edge of the bed, and sip water before you step out. If you experience nighttime hypertension (a sideeffect of midodrine), take the last dose at least four hours before bedtime.
Sweating Problems
Both too much and too little sweating can be distressing. For hypersweating, topical glycopyrrolate works like a gentle offswitch for sweat glands. For reduced sweating, stay hydrated, use a humidifier at night, and keep skin moisturized to avoid cracking.
Bladder & Sexual Function
Overactive bladder symptoms often respond to antimuscarinic agents like oxybutynin. Timed voidingsetting an alarm to go to the bathroom every 23hourshelps retrain the bladder. If sexual dysfunction crops up, discuss phosphodiesterase5 inhibitors (Viagra) with your doctor; theyre safe for most diabetic patients.
Lifestyle And Risks
While medications do the heavy lifting, lifestyle choices are the daily fuel that keeps you moving forward.
Intensive Glycemic Control
Maintaining an A1c under 7% isnt just a numberits the single most powerful tool against nerve damage. Continuous glucose monitors (CGMs) give you realtime feedback, helping you avoid spikes that accelerate neuropathy.
BloodPressure & Cholesterol Targets
Follow the ACC/AHA guidelines: keep systolic pressure <130mmHg and LDLC under 70mg/dL if you have established cardiovascular disease. Statins and ACE inhibitors not only protect the heart but also improve nerve blood flow.
Exercise
Lowimpact activitieswalking, swimming, stationary cyclingboost circulation without overstressing your joints. Add balance drills (standing on one foot, TaiChi) to reduce fall risk caused by orthostatic dizziness.
Smoking & Alcohol
Both worsen oxidative stress on nerves. If you smoke, consider nicotine replacement or counseling; for alcohol, limit to occasional glassesexcess can exacerbate neuropathy.
Daily Checklist
- Check blood glucose first thing in the morning.
- Take prescribed meds with food (if required).
- Drink a glass of water before standing.
- Record any new symptoms in a journal.
- Schedule a followup visit every 36months.
Benefits vs Risks
Every treatment has a tradeoff. Understanding both sides helps you make informed decisions with your healthcare team.
ShortTerm Benefits
- Improved blood pressure stability fewer falls.
- Faster gastric emptying less nausea, better nutrition.
- Reduced excessive sweating comfort and confidence.
Potential Risks
- Midodrine may cause high blood pressure while lying down.
- Metoclopramide carries a rare risk of tardive dyskinesia.
- Fludrocortisone can lead to fluid retention and low potassium.
Monitoring Plan
Set up a simple schedule:
- Blood pressure: morning and evening.
- Electrolytes: every 3months if on fludrocortisone.
- Neurological checkin: ask your doctor about any new tingling or gait changes.
When you weigh pros and cons on paper, the decision feels less like a gamble and more like a collaborative plan.
Real World Stories
Stories turn data into something you can relate to. Below are a few snapshots from people whove walked this path.
Johns Journey
John, 62, struggled with dizzy spells that knocked him off his feet at family gatherings. After a tilttable test confirmed orthostatic hypotension, his doctor started him on lowdose midodrine and prescribed compression stockings. Within two weeks, John could stand up for a full minute without feeling lightheadeda huge win for his confidence.
Marias Meal Plan
After months of unpredictable nausea, Maria learned that eating six tiny meals a day, avoiding fats, and adding metoclopramide reduced her gastroparesis symptoms by 70%. I stopped fearing dinner, she says, smiling.
Support Groups
Online forums like the Diabetes Neuropathy Community provide a space to share tips, ask questions, and celebrate small victories. According to a 2023 study, patients who actively participated in peer groups reported 30% higher treatment adherence.
When To Seek Care
Know the red flags that call for immediate medical attention:
- Sudden fainting episodes or loss of consciousness.
- Severe, persistent vomiting or inability to keep food down.
- Chest pain, palpitations, or unexplained rapid heart rate.
- Worsening foot ulcers (neuropathy often coexists with peripheral nerve loss).
When you notice any of these, call your doctor or go to the emergency department. Early intervention can prevent complications from spiraling.
Trusted Helpful Resources
For deeper dives, these reputable sources keep the information uptodate:
Conclusion
Living with diabetic autonomic neuropathy can feel like navigating a maze, but with the right foundationtight glucose control, symptomtargeted medications, and sensible lifestyle tweaksyou can turn many of those deadends into clear pathways. Remember, every step you take, from sipping water before standing to joining a support forum, adds up to a life thats steadier, more comfortable, and full of hope. If you have questions, share your thoughts in the comments or reach out on a trusted diabetes community. Together were stronger, and together well keep moving forward.
For guidance on navigating insurance and support options for specialty therapies that may be relevant if you face complex treatment decisions, see Exondys 51 insurance.
FAQs
What lifestyle changes help manage diabetic autonomic neuropathy?
Small, frequent meals, staying well‑hydrated, avoiding rapid position changes, wearing compression stockings, and regular low‑impact exercise can all improve symptoms.
How does tight blood‑sugar control affect autonomic neuropathy?
Maintaining an A1C below 7 % reduces the progression of nerve damage and often lessens the severity of symptoms such as dizziness and gastroparesis.
Which medications are commonly used for orthostatic hypotension?
Midodrine and fludrocortisone are first‑line drugs; they raise blood pressure when standing but require monitoring for supine hypertension.
What are the treatment options for diabetic gastroparesis?
Prokinetic agents like metoclopramide or domperidone, dietary modifications (low‑fat, low‑fiber meals), and sometimes gastric electrical stimulation are used.
When should I seek urgent medical care for autonomic neuropathy symptoms?
Call your doctor or go to the ER if you experience fainting, severe vomiting, sudden chest pain, rapid heart rate, or worsening foot ulcers.