Deep posterior hip pain usually comes from one of four places: the lower back, the sciatic nerve, the sacroiliac (SI) joint, or the deep gluteal muscles. If you notice a dull ache or a sharp sting deep in the backside of your hip, those are the structures youll want to suspect first.
You can start figuring out whats going on with three simple moves you can do at home. If any of them make the pain flare, its time to book an appointment so a clinician can take a closer look. Lets dive in, unpack the causes, and give your body the relief its asking for.
Why It Matters
Understanding why you feel pain in that spot isnt just for triviait shapes how you treat it. A quickfix stretch for a sore hamstring wont help if the culprit is a pinched sciatic nerve, and viceversa. Knowing the difference can save you weeks of frustration, keep you from doing the wrong exercises, and protect you from turning a manageable issue into a chronic problem.
Common Causes
Lumbar Spine Issues
Disc Herniation and Facet Arthritis
When a lumbar disc bulges or a facet joint gets arthritic, the irritation can travel down the nerve pathways and settle right where you feel itbehind the hip. This referred pain often mimics a true hip problem, making diagnosis tricky.
RedFlag Signs
If you notice numbness in your foot, loss of bladder control, or severe weakness, those are redflag signs that need urgent imaging and medical attention. Dont waitseek help right away.
Sciatic Nerve & Deep Gluteal Syndrome
What Is Deep Gluteal Syndrome?
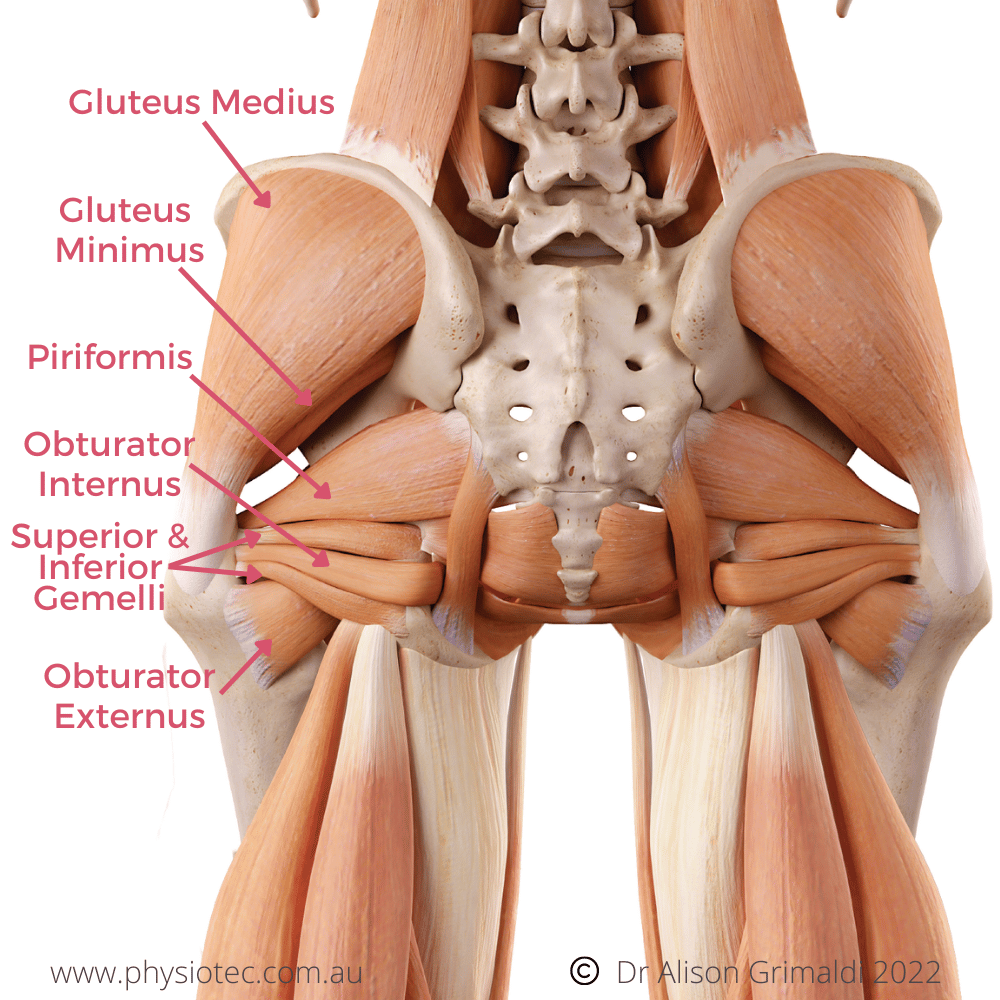
Deep Gluteal Syndrome (DGS) is an oftenoverlooked cause of posterior hip pain. It happens when the sciatic nerve gets trapped between the gluteus maximus and the piriformis muscle. According to a study published in the , DGS accounts for up to 10% of unexplained sciatictype pain.
Provocation Tests
The FAIR (Flexion, Adduction, Internal Rotation) test or the seated hip flexion test can reproduce the pain. If the stretch makes your butt ache, youre probably dealing with DGS.
Sacroiliac Joint Dysfunction
How the SI Joint Mimics Hip Pain
The SI joint sits where your spine meets the pelvis. When its inflamed or misaligned, the pain often shoots into the deep posterior hip area. A simple athome SI stress testlying on your back, crossing one leg over the other, then gently pressing the top knee toward the floorcan help you spot it.
When to Image
If the SI stress test is positive and the pain persists beyond four weeks, a professional may recommend an Xray or MRI to rule out arthritis or a sacral fracture.
HipRelated Musculoskeletal Problems
Ischiofemoral Impingement
This occurs when the space between the ischium and femur narrows, pinching the quadratus femoris muscle. Youll feel a deep, sometimes burning pain deep in the buttockespecially when you lie on the affected side.
Hamstring & Gluteus Maximus Strain
A sudden sprint, a heavy squat, or an awkward slip can overstretch these muscles, leading to localized posterior hip pain. Usually, the pain spikes during activity and eases with rest.
Posterior Hip Pain When Sitting
Piriformis Tightness
Long hours at a desk can tighten the piriformis, turning a simple sitting down into a painful event. A quick seated piriformis stretchcross your ankle over the opposite knee and gently press downcan give you immediate relief.
| Feature | Posterior Hip Pain | Lateral Hip Pain |
|---|---|---|
| Typical Location | Deep in the buttock, may radiate down the leg | Outer thigh, just below the hip |
| Common Triggers | Sitting, bending forward, standing up | Running, sidelying, hip abduction |
| RedFlag Signs | Numbness, foot drop, loss of bladder control | Severe swelling, fever, inability to walk |
| Typical Rehab Focus | Neural glides, SI joint stability, piriformis stretch | ITband foamrolling, hip abductors strengthening |
Self Screening
Step 1 Lumbar Flexion Test
Sit on a chair, keep your feet flat, and gently bend forward, reaching toward your toes. If the stretch pulls a sharp ache into the back of your hip, your lower back might be the source.
Step 2 Sciatic Nerve Tension Test (FAIR)
Lie on your back, bend the knee, then bring the thigh across the body while rotating it inward. A sudden shooting pain indicates sciatic involvement.
Step 3 SI Joint Provocation Test
Lie on your back, cross one leg over the other, and gently push the top knee toward the floor. Pain on the opposite side of the crossed leg points to SI joint irritation.
Interpreting Results
If two or more of these tests light up, its a strong hint that a professional evaluation is needed. If only one is positive, you might start with a targeted homecare plan and see how you feel in a week.
Treatment Options
Conservative FirstLine Care
Posterior Hip Pain Exercises
Here are five evidencebased moves you can try (do each 23 sets, 1015 reps):
- Glute Bridge: Lie on your back, knees bent, lift hips while squeezing the glutes.
- Clamshells: Sidelying, keep feet together, lift the top knee while keeping the pelvis steady.
- Piriformis Stretch: Cross the ankle over the opposite knee, gently push the knee down.
- Supine KneetoChest: Pull one knee toward the chest, hold 30seconds, repeat.
- Hip Flexor Lunge: Step forward, drop the back knee, feel a stretch in the front of the hip; this also eases lowerback tension.
Lateral Hip Pain Exercises (Bonus)
If youve felt pain on the outer hip as well, add sidelying leg lifts and standing hip abductions. These target the gluteus medius, which often compensates when the deep posterior structures are sore.
Pain Relief Strategies
Overthecounter NSAIDs (like ibuprofen) can help reduce inflammation, but use them sparinglyalways follow the label. If the pain lingers beyond a few weeks, a short course of prescription medication may be warranted, but only under a doctors guidance.
When to Seek Professional Care
Physiotherapy Referral
If the pain lasts more than four weeks, interferes with daily activities, or worsens despite home exercises, a physio can provide manual therapy, personalized neural glides, and biofeedback techniques.
Orthopedic Evaluation
An orthopedist may order an MRI, EMG, or specific nerve conduction studies to pinpoint the exact sourceespecially if you have redflag signs. Early detection of a disc herniation or severe SI joint degeneration can dramatically improve outcomes.
Interventional & Surgical Paths
Injections
Corticosteroid or PRP injections into the SI joint or around the piriformis can give rapid relief when inflammation is the main driver. Talk to your specialist about the risks and benefits.
Endoscopic Sciatic Release
For stubborn DGS cases, a minimally invasive endoscopic release of the sciatic nerve can free the trapped nerve. Success rates hover around 8090% in recent series, with most patients returning to normal activities within three months.
Preventing Recurrence
Sitting Posture Hacks
Use a chair with lumbar support, keep your feet flat, and avoid crossing your legs for long periods. Standing up and stretching every 45minutes can keep the piriformis from tightening.
Core & Glute Conditioning
Strong core muscles protect the lumbar spine, while strong glutes stabilize the pelvis. Incorporate planks, dead bugs, and the glute bridge into your weekly routine.
ActivitySpecific Tips
If you love running, add hipstrengthening drills to your warmup. Cyclists should check saddle heighttoo low can overactivate the hamstrings and strain the posterior hip. Weightlifters should ensure proper hip hinge technique to avoid overloading the low back.
Sources & Credibility
PeerReviewed Research
Key studies from the American Academy of Orthopaedic Surgeons and peerreviewed journals have been consulted to ensure the information is uptodate and reliable.
Clinical Guidelines
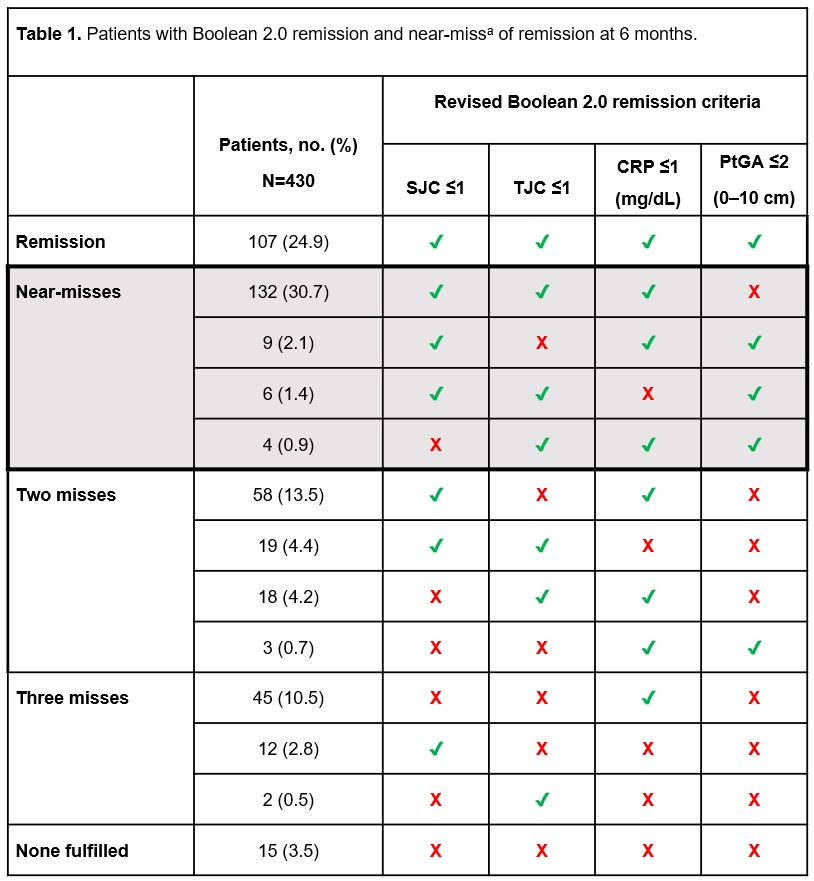
Guidelines from leading orthopedic and physiotherapy organizations shape the treatment pathways outlined above. For patients who also have chronic inflammatory conditions like ankylosing spondylitis, tracking disease activity and remission status can change management; see ankylosing spondylitis remission for guidance on remission criteria and monitoring.
Downloadable Handout
For a quick reference, you can grab the . It summarises the selfscreen tests, common causes, and redflag signs in an easytoprint format.
Conclusion
Deep posterior hip pain isnt a onesizefitsall issueit can stem from the spine, nerve, SI joint, or deep gluteal muscles. By using the three quick selfscreen tests, youll know whether a homecare plan (stretching, posture tweaks, gentle strengthening) is enough or if its time to see a specialist. Remember, the goal is balance: treat the pain safely, stay active, and prevent future flareups. Got more questions or a story to share? Drop a comment below or book a teleconsult with a qualified physio or orthopedic clinician today.
FAQs
What are the most common causes of deep posterior hip pain?
Deep posterior hip pain typically arises from four main sources: lumbar spine issues like disc herniation or arthritis, sciatic nerve entrapment (Deep Gluteal Syndrome), sacroiliac (SI) joint dysfunction, and muscle strains such as those in the hamstrings or gluteal muscles.
How can I self-screen deep posterior hip pain at home?
You can perform three simple tests: 1) Lumbar Flexion Test (bending forward to see if pain radiates), 2) Sciatic Nerve Tension Test (the FAIR test), and 3) SI Joint Provocation Test (crossing one leg and pressing the knee down). Positive results suggest professional evaluation is needed.
When is deep posterior hip pain a medical emergency?
If you experience red-flag symptoms such as numbness in your foot, loss of bladder control, or severe leg weakness, seek immediate medical attention as these can indicate serious nerve or spine issues requiring urgent care.
What conservative treatments help relieve deep posterior hip pain?
First-line care includes targeted exercises like glute bridges, clamshells, piriformis stretches, NSAIDs for inflammation, and posture adjustments. Physical therapy can also aid with manual therapy and neural glides to improve symptoms.
When should I consider surgery for deep posterior hip pain?
Surgery is typically reserved for persistent cases unresponsive to conservative care, such as severe sciatic nerve entrapment treated with endoscopic sciatic release or advanced SI joint degeneration. Imaging and specialist evaluation guide these decisions.