At first, I thought it was nothing more than a weird muscle spasm you see in movies. Then I met a friend whose brother was in the ICU, and the doctors kept mentioning decorticate and decerebrate posturing terms that felt like they belonged on a scifi alien manual. The truth is, these postures are serious signals from the brain, and understanding decorticate vs decerebrate posturing causes can make a huge difference in how quickly help arrives.
In the next few minutes, Ill walk you through what each posture looks like, why one is usually worse than the other, the brain structures involved, and even a handy mnemonic to keep it all straight. Think of it as a quick chat over coffee, with a few reallife stories and a sprinkle of science to keep things clear.
What They Mean
Decorticate Posturing The Flex
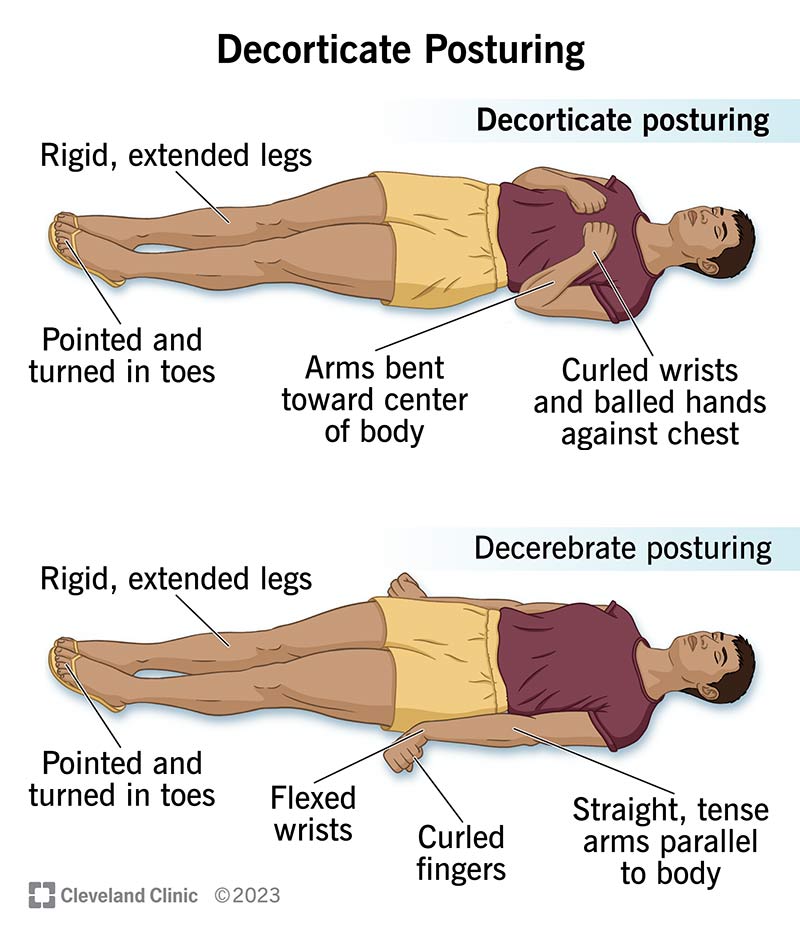
When a patients arms are flexed (bent at the elbows) and the wrists are tucked in, while the legs are extended, we call that decorticate posturing. Its like the body is trying to curl up into a protective ball, but the brain is sending mixed signals.
Decerebrate Posturing The Extend
Decerebrate posturing looks almost the opposite: arms and legs are both extended, with the wrists flexed and the fingers pointing down. This stiff, straightarmed pose suggests a deeper level of brain injury.
Why the Difference Matters
Doctors use these postures as a fast, visual red flag to gauge where the damage lies inside the skull. Knowing the cause helps them decide whether surgery, medication, or other interventions might turn the tide. For example, if imaging suggests a cortical source, targeted neurosurgical evaluation may be prioritized.
Quick Visual Cue
| Posture | Typical Body Position | Underlying Level of Injury |
|---|---|---|
| Decorticate | Arms flexed, legs extended | Above the red nucleus (cortical or subcortical) |
| Decerebrate | Arms & legs extended, wrists flexed | At or below the red nucleus (brainstem) |
Root Causes
Where the Damage Happens
Think of the brain as a threestory building. The first floor is the brainstem, the second floor is the thalamus and basal ganglia, and the top floor is the cerebral cortex. Decorticate posturing typically results from injuries to the second or top floors, while decerebrate posturing points to problems on the first floor.
What Causes Decorticate Posturing?
Common culprits include:
- Severe traumatic brain injury (TBI) large contusions or hematomas pressing on the cortex.
- Intracerebral hemorrhage especially in the basal ganglia or internal capsule.
- Large ischemic strokes affecting the thalamus or surrounding white matter.
- Prolonged seizures (status epilepticus) intense cortical firing can trigger the flexed posture.
What Causes Decerebrate Posturing?
This posture usually signals damage deeper down:
- Massive brainstem stroke hitting the pons or midbrain.
- Diffuse axonal injury where the brain shakes so hard that the brainstem fibers tear.
- Severe hypoxia or anoxia neardrowning, cardiac arrest, or carbon monoxide poisoning.
- High cervical spinal cord injury can mimic brainstem shutdown.
Survival Rate Snapshot
On average, patients who show decorticate posturing have a , depending on how quickly the underlying cause is treated. Decerebrate posturing, because it implicates the brainstem, is associated with a higher mortality often exceeding 60% in severe cases.
Which Is Worse
Understanding the Severity Gap
Simply put, decerebrate posturing is usually worse. The brainstem houses vital centers for breathing, heart rate, and consciousness. When those centers are compromised, the body loses its ability to regulate the basics of life. Decorticate posturing, while serious, indicates that some brainstem function is likely still intact.
Exceptions to the Rule
Medicine loves exceptions. Some patients with massive edema and decerebrate posture have turned around after aggressive decompressive surgery. Conversely, a deep cortical bleed causing decorticate posture can be fatal if not evacuated promptly. The key is not to assume fate, but to act fast.
How To Diagnose
Imaging the Injury
A noncontrast CT scan is the first line it shows hemorrhage, fractures, and large mass effects. For subtle brainstem lesions, an MRI (especially diffusionweighted imaging) offers better detail. Early imaging protocols used in stroke or TBI pathways often determine the urgency of interventions like thrombectomy or craniotomy.
Neurological Exam Tips
Beyond the posture itself, watch the pupils: unequal or nonreactive pupils often accompany decerebrate signs. Check gag reflexes and respiratory patterns irregular breathing can hint at brainstem involvement.
Lab Clues
Severe hypoxia will show low blood oxygen and possible lactic acidosis. Elevated CO can worsen cerebral edema, pushing a patient from decorticate into decerebrate.
Diagnostic Flowchart
| Observed Posture | Check First | Likely Injury Zone |
|---|---|---|
| Decorticate | CT head for cortical bleed/contusion | Above red nucleus (cortex, thalamus) |
| Decerebrate | CT/MRI brainstem; ABG for hypoxia | At/below red nucleus (brainstem) |
Treatment Basics
Immediate Steps
Airway, breathing, circulation the ABCs never change. If the posture is due to increased intracranial pressure (ICP), start hyperventilation (briefly), administer osmotic agents like mannitol, and consider a hypertonic saline infusion.
Targeted Interventions
- Surgical decompression removing a hematoma or relieving a skull fracture can reverse posturing.
- ICP monitoring placed after stabilizing the airway, it guides ongoing therapy.
- Seizure control benzodiazepines or barbiturates for status epilepticus that may have triggered decorticate posture.
- Neuroprotective strategies maintaining normoxia, normocapnia, and optimal perfusion pressure.
Rehabilitation Outlook
Even when the acute crisis passes, patients may need weeks to months of physical, occupational, and speech therapy. The earlier you know which area of the brain was injured, the more tailored the rehab plan can be. For families navigating long recoveries, resources about specific neurologic conditions can help set expectations and connect with support for example, reading up on Rett syndrome types can illustrate how different injury patterns map to varying long-term needs in other neurodevelopmental contexts.
Memory Aid
Decorticate vs Decerebrate Mnemonic
Heres a quick rhyme I like to use when Im on a night shift:
C for Cortical, Flex the arms, B for Brainstem, Extend the charms.
Its simple: C = Cortical (or above the red nucleus) arms flex; B = Brainstem (or below the red nucleus) arms extend.
Graphic Suggestion
If youre a visual learner, sketch two stickfigures side by side, label the brain structures, and write the mnemonic underneath. It sticks in the mind faster than a paragraph of prose.
Real Stories
Case 1: The Young Driver
James, 28, was in a highspeed collision. He arrived with a massive left temporal lobe contusion. The ER team noted decorticate posturing. An urgent CT showed a 3cm epidural hematoma pressing on the motor cortex. Within an hour, surgeons performed a craniotomy and evacuated the clot. James recovered enough to walk a few weeks later, though he now has mild lefthand weakness. His story underscores how decorticate posture often signals a surgicallytreatable bleed.
Case 2: The Silent Stroke
Maria, 62, woke up with a sudden, slurred speech and a stiff, extended posture classic decerebrate. A CT scan revealed a basilar artery occlusion, a devastating brainstem stroke. Even with aggressive thrombolysis, her brainstem damage was extensive, and she required ventilator support. Marias family was prepared for a tough road, illustrating why decerebrate posturing is such a grave warning sign.
TakeAway Nuggets
- Rapid imaging can change a decorticate scenario from fatal to survivable.
- Decerebrate signs demand immediate stabilization and often a discussion about goals of care.
- Both patients benefited from clear communication with the medical team knowing the cause gave families a roadmap.
Quick FAQ (Embedded in the Text)
What causes decorticate posturing?
Injury above the red nucleus typically cortical contusions, basal ganglia hemorrhages, large strokes, or prolonged seizures.
What causes decerebrate posturing?
Damage at or below the red nucleus brainstem strokes, diffuse axonal injury, severe hypoxia, or high cervical spinal cord lesions.
Which posture indicates a worse prognosis?
Decerebrate posturing, because it reflects brainstem dysfunction, which controls essential lifesustaining functions.
Is there a simple way to remember the difference?
Yes C for Cortical (Flex), B for Brainstem (Extend). Its a handy mnemonic that sticks.
Can a patient switch from decorticate to decerebrate?
Unfortunately, yes. Worsening edema or a new brainstem bleed can shift the posture, signaling rapid clinical decline.
What is the typical survival rate for decorticate posturing?
About 3040% survive to discharge, though outcomes vary widely with cause and treatment speed.
Does seizure activity cause decorticate posture?
Prolonged seizures (status epilepticus) can fire the cortex intensely enough to produce decorticate flexion.
Conclusion
Understanding decorticate vs decerebrate posturing causes isnt just academic; it can be the difference between a timely surgical rescue and a heartbreaking wait for the inevitable. Decorticate points to cortical or subcortical injury serious, but often treatable. Decerebrate suggests brainstem involvement, which usually carries a grimmer outlook.
When you or a loved one notice these postures, call emergency services immediately. Share the mnemonic C for Cortical, B for Brainstem with first responders it helps them convey the urgency fast. And if youve experienced this yourself, please consider sharing your story in the comments; your voice could guide someone else through a scary moment.
Stay curious, stay compassionate, and remember: knowledge is one of the strongest tools we have in the fight against brain injury.
FAQs
What causes decorticate posturing?
Injury above the red nucleus, such as cortical contusions, basal ganglia hemorrhages, large strokes, or prolonged seizures.
What causes decerebrate posturing?
Damage at or below the red nucleus, including brainstem strokes, diffuse axonal injury, severe hypoxia, or high cervical spinal cord lesions.
Which posture indicates a worse prognosis?
Decerebrate posturing, because it reflects brainstem dysfunction, which controls essential life-sustaining functions.
Can a patient switch from decorticate to decerebrate?
Yes, worsening edema or a new brainstem bleed can shift the posture, signaling rapid clinical decline.
Does seizure activity cause decorticate posture?
Prolonged seizures (status epilepticus) can fire the cortex intensely enough to produce decorticate flexion.