Ever felt that tight, cantburp sensation after a big meal or struggled to swallow a piece of toast? Chances are, the tiny gatekeeper at the back of your throat the cricopharyngeus muscle is trying to tell you something. In the next few minutes, well walk through exactly what this muscle does, why it sometimes misbehaves, and the best ways doctors set it right. No jargon, just friendly, bitesize facts you can actually use.
Anatomy & Physiology
Where is the cricopharyngeus muscle?
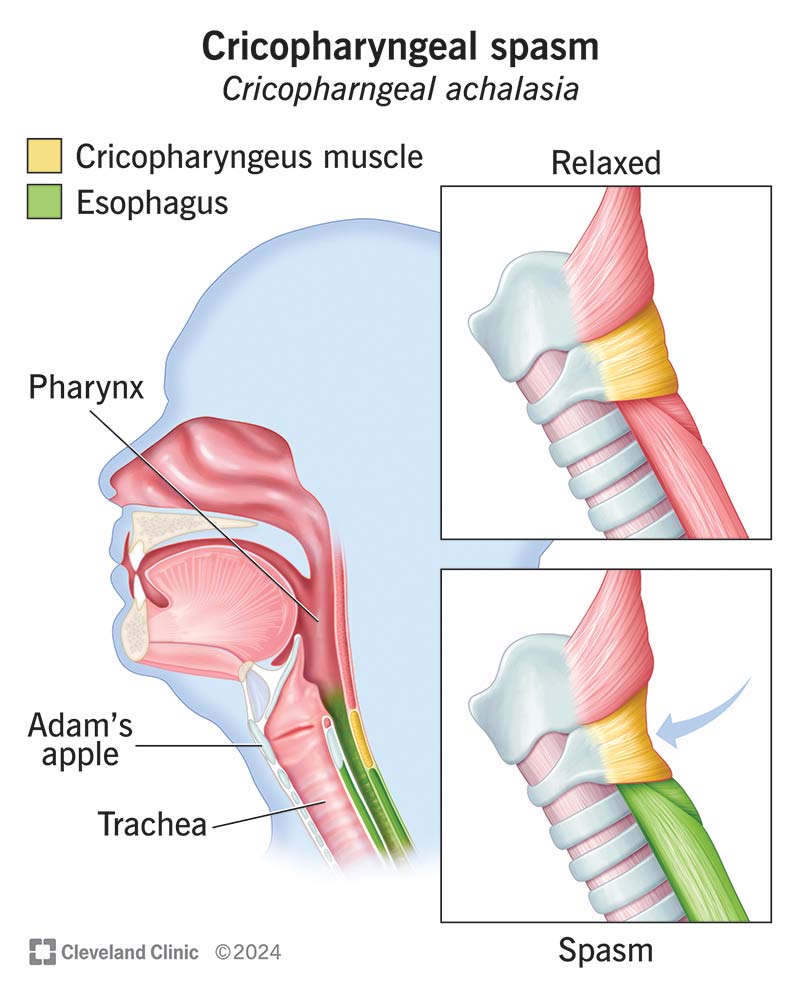
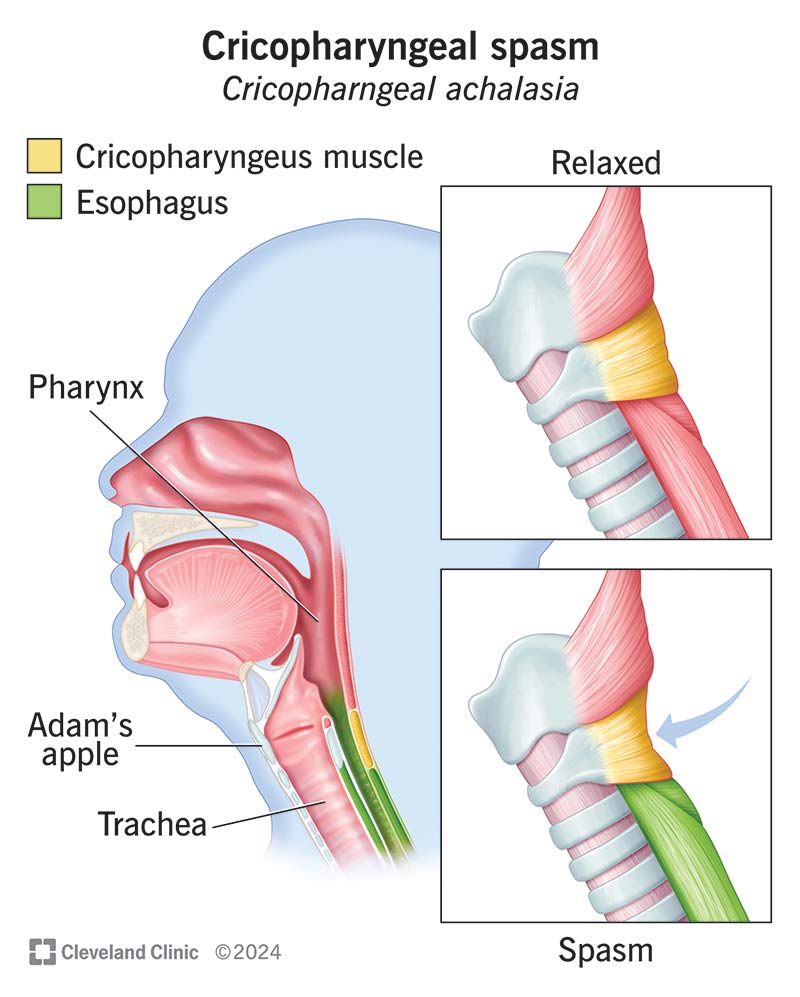
The cricopharyngeus sits just below the Adams apple, forming a ring around the uppermost part of the esophagus. Think of it as the latch on a door that usually stays closed but swings open when you swallow. Its location is easy to picture on a neck CT scan youll see a thin, muscular band hugging the airway and esophagus.
How does it work with the thyropharyngeus?
The cricopharyngeus doesnt act alone. Below it, the thyropharyngeus muscle pulls food down while the cricopharyngeus relaxes to let it pass. Imagine a tandembike: the thyropharyngeus pedals forward (pushes) and the cricopharyngeus releases the brake. Together they create a smooth, coordinated swallow.
What creates the highpressure zone?
Because its made of striated (skeletal) muscle, the cricopharyngeus maintains a resting tone that keeps air and food from leaking back into the throat. Manometric studies show a pressure of about 3040mmHg at rest enough to keep the airway sealed yet low enough to open easily when a swallow signal hits the brainstem.
Expert Insight
According to a recent review in (2024), the cricopharyngeus is considered the gatekeeper of the upper esophageal sphincter, highlighting its central role in safe swallowing.
Nerve Supply
Which nerves talk to the cricopharyngeus?
The muscle gets its commands mainly from the vagus nerve (CNX), especially via the recurrent laryngeal branch and the pharyngeal plexus. These nerves tell the cricopharyngeus when to relax and when to snap shut.
How do reflexes keep swallowing safe?
When you take a bite, sensory receptors in the mouth send a signal to the brainstem. The nucleus ambiguus processes that cue and fires a rapid openthegate command to the cricopharyngeus. The whole sequence happens in less than a second pretty impressive for a reflex!
When nerves get mixed up common neuropathic causes
Injury to the vagus nerve can come from a stroke, ALS, neck surgery, or even a harsh coughing spell. When the signal falters, the cricopharyngeus may stay too tight (spasm) or become too lax (weakness), leading to swallowing trouble.
Case Vignette
Emily, a 58yearold teacher, noticed food sticking after a thyroidectomy. A speechlanguage pathologist ran a brief EMG and discovered reduced vagal input to her cricopharyngeus. Targeted therapy and a botox injection later, she was back to her favorite salsadancing meals.
When It Malfunctions
| Dysfunction | Core Problem | Typical Symptoms | Imaging / Test |
|---|---|---|---|
| Cricopharyngeal spasm | Failure to relax during swallow | Food feels stuck, throat pressure | VFSS, manometry |
| Cricopharyngeal bar | Fibrous thickening (UCLA bar) | Dysphagia, sensation of a ridge | CT, esophagram |
| Retrograde CPD (Noburp) | Incomplete opening on belch | Inability to burp, bloating | Video endoscopy |
| Neurogenic paresis | Nerve damage | Weak swallow, aspiration risk | EMG, nerve conduction |
How to spot the problem redflag symptoms
If youre coughing after meals, losing weight unintentionally, or feel like food is getting stuck every few minutes, its time to get evaluated. These arent just minor annoyances; they can signal a serious cricopharyngeus dysfunction.
Diagnostic toolbox
Doctors often start with a barium swallow (quick, visual), then may move to highresolution manometry (measures pressure changes). A CT scan of the neck cricopharyngeus muscle CT can reveal a bar or structural abnormality. Endoscopy lets them look directly at the muscles surface.
When is it just a sore throat vs. true dysfunction?
A sore throat from a cold usually improves in a week and lacks the swallowingspecific signs above. Persistent trouble after the infection clears? Thats a clue the cricopharyngeus might need a closer look.
Treatment Options
NonSurgical Approaches
Botox injection
Botulinum toxin temporarily relaxes the muscle by blocking nerve signals. Studies show a 7085% success rate for reducing spasms, and the effect usually lasts 36 months. The downsides? A brief period of mild dysphagia or voice hoarseness while the toxin takes effect.
Swallowing therapy & musclerelaxation exercises
Speechlanguage pathologists teach maneuvers like the Mendelsohn technique (hold the swallow) and the Shaker exercise (head lifts to strengthen the suprahyoid muscles). These help retrain the cricopharyngeus to open more smoothly.
Realworld story
Mike, a 45yearold marathon runner, tried Botox with decent relief but felt off after a month. He added a sixweek program of Shaker exercises, and his swallowing confidence returned fully no more choking on energy gels.
Surgical Options
Cricopharyngeal myotomy
When injections or therapy fail, surgeons may cut the muscle fibers (myotomy) to permanently reduce tension. It can be done endoscopically or via a small neck incision. Success rates hover around 90% for severe bars, though voice changes or temporary reflux can occur.
Dilatation & endoscopic radial incision
For earlystage bars, a pneumatic dilator or a radial incision using a laser can gently stretch the muscle without cutting it fully. This approach often shortens recovery time.
Choosing the right path
Think of treatment like picking a route on a map. If the problem started after a nerve injury, doctors may try Botox first. If the muscle is thickened (a bar), a myotomy might be the most direct route. A simple flowchart can guide you:
- Is the issue neurogenic? Try therapy + Botox.
- Is there a visible bar on CT? Consider dilatation or myotomy.
- Did nonsurgical measures fail? Move to surgery.
Expert Consensus
The American Academy of Otolaryngologys 2024 clinical guideline recommends a stepwise approach, emphasizing patientcentered decision making and multidisciplinary input from ENT surgeons, gastroenterologists, and speech therapists.
Living After Treatment
Diet modifications
During the first few weeks, stick to soft foods (mashed potatoes, yogurt) and avoid tough meats or crusty bread. Thickened liquids can also reduce the risk of aspiration while the muscle heals.
Voice & breathing considerations
Because the cricopharyngeus shares nerves with the vocal cords, any procedure can momentarily affect voice quality. If you notice hoarseness lasting more than a week, reach out to a laryngologist most changes are temporary.
Followup schedule
After Botox, a followup at 46 weeks checks the effect and plans for possible repeat injection. Postmyotomy patients typically get a repeat manometry at 3 months to confirm the pressure zone has normalized.
Support resources
Online communities like the Dysphagia Support Group on Facebook or apps such as SwallowSmart let you share experiences, ask questions, and stay motivated. Knowing youre not alone makes the recovery journey far less lonely.
Conclusion
The cricopharyngeus muscle may be small, but it plays a starring role in every swallow, every belch, and every quiet moment between a sip of water and a laugh. When it works, you never notice it; when it doesnt, the world can feel unexpectedly clogged. By understanding its anatomy, nerve supply, and the spectrum of cricopharyngeus muscle dysfunction, youre empowered to recognize warning signs early and seek the right care whether thats a targeted Botox shot, a set of therapistguided exercises, or, in more stubborn cases, a precise surgical myotomy.
If youve experienced any of the symptoms described, dont wait. Talk to an ENT specialist or a speechlanguage pathologist. Their expertise, combined with the proven treatments outlined here, can help you get back to enjoying meals, conversations, and even that satisfying burp after a fizzy drink. And remember, youre not navigating this alone theres a whole community of professionals and fellow patients ready to support you every step of the way.
For readers specifically struggling with the inability to burp and related retrograde symptoms, consider learning more about practical approaches to retrograde cricopharyngeus dysfunction and the common inability to burp presentations as part of the diagnostic conversation with your clinician.
FAQs
What is the cricopharyngeus muscle and where is it located?
The cricopharyngeus muscle is a circular band of striated muscle that forms the upper esophageal sphincter. It lies just below the Adam’s apple, encircling the top of the esophagus.
How does the cricopharyngeus work together with the thyropharyngeus?
During a swallow, the thyropharyngeus contracts to push food downward while the cricopharyngeus relaxes to open the sphincter, allowing the bolus to pass smoothly.
What are the most common dysfunctions of the cricopharyngeus muscle?
Typical problems include cricopharyngeal spasm (failure to relax), cricopharyngeal bar (fibrous thickening), retrograde CPD (“no‑burp” syndrome), and neurogenic paresis from vagus nerve injury.
When is Botox injection recommended for cricopharyngeus issues?
Botox is usually tried first for neurogenic spasm or mild hypertonicity. The toxin temporarily relaxes the muscle, providing symptom relief for 3‑6 months before repeat treatment may be needed.
What should a patient expect after a cricopharyngeal myotomy?
After myotomy, most patients experience rapid improvement in swallowing. Recovery involves a soft‑diet phase, voice monitoring, and a follow‑up manometry around three months to confirm pressure normalization.