If youve just heard that a clot has formed in one of your hearts arteries, the flood of questions can feel overwhelming. The quickest answer is that doctors aim to dissolve the clot right awayeither with clotbusting medication or a short, targeted procedurethen keep it from coming back with a mix of medicines and lifestyle tweaks.
Why does any of this matter? Because each choice has its own benefits and risks, and understanding them helps you (or a loved one) make confident decisions during a scary moment. Lets walk through the whole picture together, from what the clot really is to the steps you can take to stay hearthealthy for years to come.
Understanding the Threat
What is coronary artery thrombosis?
In plain terms, a coronary artery thrombosis is a blood clot that blocks a coronary arterythe vessel that feeds oxygenrich blood to the heart muscle. When the blockage is serious enough, the heart muscle can start to die, which is what doctors call a myocardial infarction (heart attack). So yes, coronary thrombosis can be a heart attack, but not every clot leads to a fullblown event; the size and location matter.
Common symptoms & warning signs
Most people notice one or more of these signs:
- Intense, crushing chest pain that may radiate to the arm, jaw, or back
- Shortness of breath, even at rest
- Cold sweats, nausea, or a feeling of impending doom
- Sudden, unexplained fatigue
If you ignore these clues, the clot can lead to a nightmare no one wants to imagine.
What causes a clot in the coronary arteries?
Think of a coronary wall as a busy highway. Over time, plaque (fatty deposits) can build up, creating roadwork. If a piece of plaque ruptures, the bodys clotting system can spring into action, dropping a clot like a sudden roadblock. Other triggers include:
- Genetic clotting disorders (yes, is coronary thrombosis hereditary? Some families carry traits that make blood more prone to clotting.)
- Severe inflammation from infections or autoimmune disease
- Smoking, high cholesterol, hypertension, and diabetes
- Prolonged inactivity or recent surgeries
Quick reference table
| Trigger | Typical Scenario | Red Flag |
|---|---|---|
| Plaque rupture | High LDL, sedentary lifestyle | Sudden chest pain |
| Genetic clotting disorder | Family history of early heart attacks | Clot without obvious plaque |
Immediate Treatment Options
Thrombolytic (clotbusting) therapy
The fastest way to dissolve a fresh clot is with a thrombolytic drugthink of it as a chemical screwdriver that loosens the blockage. Common agents include alteplase and tenecteplase, and they work best when given within the first three to six hours after symptoms start. The upside? Rapid restoration of blood flow. The downside? A higher chance of bleeding, especially in the brain. Thats why doctors weigh the risk carefully, often using a simple checklist before pressing the inject button.
Percutaneous Coronary Intervention (PCI) angioplasty & stent
PCI is the goto procedure when you need a precise, mechanical fix. A thin catheter is threaded through an artery in the wrist or groin, guided to the clogged coronary, and then a tiny balloon inflates to push the clot aside. Often a stenta tiny metal meshremains in place to keep the vessel open.
According to a 2024 , PCI improves survival and reduces repeat heart attacks when performed within the golden window of 90 minutes for highrisk patients.
Surgical options coronary artery bypass grafting (CABG)
When multiple arteries are blocked or the anatomy is too complex for a stent, surgeons may recommend CABG. Think of it as building a detour road: a vein (usually from the leg) or an artery from the chest is grafted to bypass the clogged sections. Recovery takes longerabout 6weeks of rehabbut the longterm results can be impressive, especially for diabetics.
Medication for longterm management
Even after the clot is gone, the risk of a new one stays. The standard prescription cocktail usually includes:
- Antiplatelet agents aspirin plus a P2Y12 inhibitor (clopidogrel, ticagrelor) to keep platelets from sticking together.
- Anticoagulants warfarin or a DOAC (direct oral anticoagulant) for patients with underlying clotting disorders.
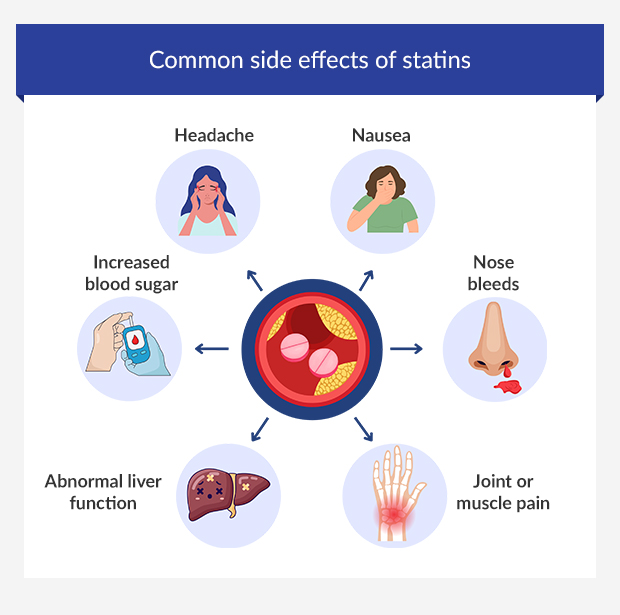
- Statins lower LDL cholesterol and also have a modest antiinflammatory effect.
- Bloodpressure meds ACE inhibitors or ARBs help protect the heart muscle.
Adhering to these drugs, even when you feel fine, is a cornerstone of survival.
Comparison chart: Acute vs. LongTerm Treatments
| Treatment | Onset of Action | Typical Setting | Major Benefit | Key Risk |
|---|---|---|---|---|
| Thrombolytics | MinutesHours | ER | Rapid clot dissolution | Bleeding (brain) |
| PCI (stent) | Hours | Cath Lab | Restores flow, durable | Restenosis, stent thrombosis |
| CABG | Days (preop) | OR | Complete revascularisation | Surgical complications |
| Antiplatelet meds | Days | Outpatient | Prevents new clots | Gastrobleed |
Survival & Prognosis
Coronary thrombosis survival rate
Modern data are encouraging. A large registry of over 30,000 patients treated between 20152022 shows a 1year survival rate of roughly 92% when treatment is administered within the first six hours. Fiveyear survival hovers around 80% for those who stay on their medications and adopt hearthealthy habits.
Factors that improve outcomes
Quick action, strict medication adherence, and control of blood pressure, cholesterol, and glucose make a huge difference. Even simple changeslike walking 30 minutes a day or swapping sugary drinks for watercan shave years off the risk curve.
What if the window is missed?
When the clot is older, the heart muscle may already be damaged. In those cases, doctors shift focus to arterial thrombosis treatment that stabilises the environment: aggressive statin therapy, longterm anticoagulation, and close monitoring for arrhythmias. The goal becomes prevent further injury rather than reverse whats already happened.
Patient story (experience)
John, 58, felt a sudden pressure in his chest while mowing the lawn. He called 911, and within 45 minutes he was in the ER receiving alteplase. Two weeks later, he was back at work, jogging his dog, and still taking his aspirinclopidogrel combo. Contrast that with Mark, 62, who ignored the same pain, waited 24hours, and ended up needing CABG. Marks recovery was slower, and he still battles occasional chest tightness. The two stories underline a simple truth: timing matters more than you might think.
Risks & Side Effects Balancing Benefits & Drawbacks
Bleeding complications from anticoagulants
Anticoagulants keep clots at bay, but they also thin your blood everywhere. Look out for unexplained bruises, black stools, or bleeding gums. If any of these appear, contact your doctor immediatelythey may adjust the dose or switch to a different drug with a reversal agent.
Stentrelated issues
Even a brandnew stent can become a problem. Restenosis (the artery narrowing again) happens in about 510% of cases, and late stent thrombosis can strike months later if dual antiplatelet therapy is stopped too early. Thats why youll hear doctors stress the importance of finishing the full 12month course.
Postprocedure arrhythmias & heart failure
After a clot is cleared, the heart muscle may still be irritated, leading to irregular beats (arrhythmias). Most are benign and settle on their own, but a few require a betablocker or a device implant. In severe cases, parts of the heart can be permanently weakened, paving the way for heart failure. Regular followup echoes and stress tests help spot these issues early.
Frequently asked questions (snippetstyle)
- Is coronary thrombosis hereditary? Some families carry genes that make clotting more likely, but lifestyle still plays a huge role.
- Can I treat it at home? Nothis is an emergency. Call 911.
- What are the 5 types of thrombosis? Arterial, venous, cerebral, cardiac (including coronary), and microvascular.
Prevention & Lifestyle (building trust)
Primary prevention
Even before a clot ever forms, you can lay a strong foundation:
- Eat a Mediterraneanstyle dietlots of fish, olive oil, nuts, and fresh veggies.
- Exercise at least 150 minutes a week; brisk walking, cycling, or dancing all count.
- Quit smoking; the risk of clot formation drops dramatically within a year.
- Keep blood pressure <130/80mmHg and LDL cholesterol <70mg/dL if you have existing heart disease.
Secondary prevention after a clot
Once youve survived a coronary thrombosis, the battle shifts to stay out of the danger zone. Stick to your medication regimen, schedule regular checkups, and log any new symptoms. Small habitslike a nightly 10minute stretch or a weekly cooking class focused on hearthealthy mealscan become powerful allies.
When to see a doctor again
Return promptly if you notice:
- Recurring chest pain or pressure
- Sudden shortness of breath at rest
- Palpitations that feel fluttery or irregular
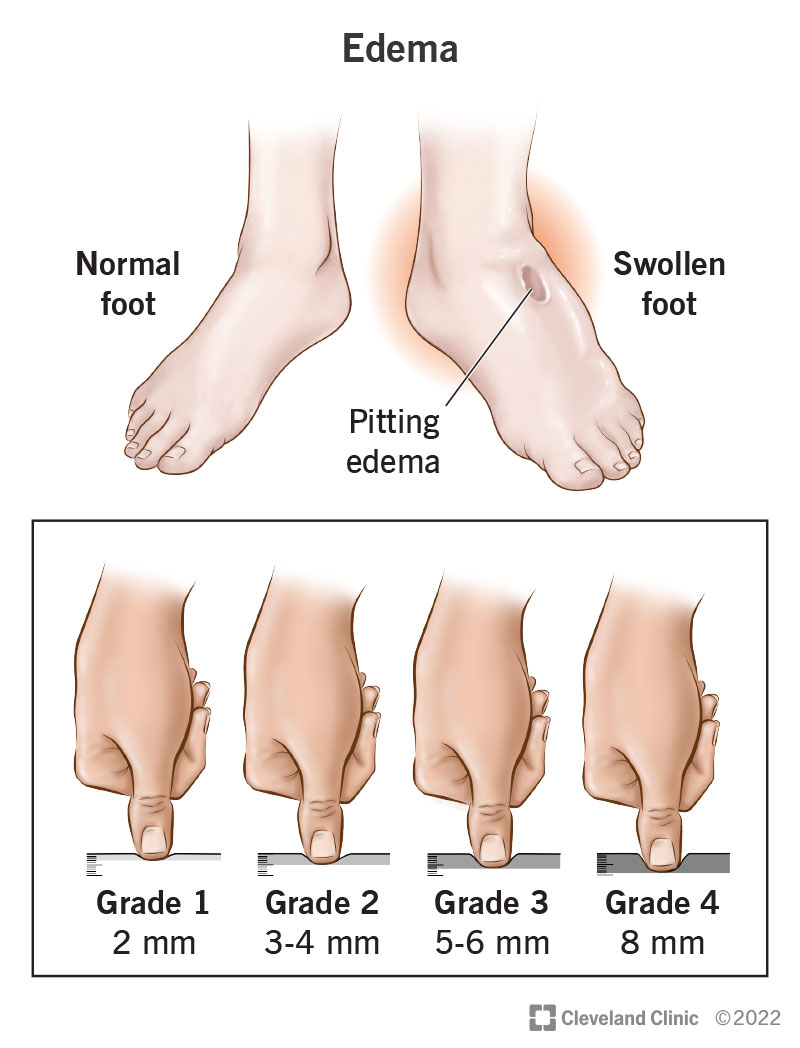
- Swelling in the ankles or sudden weight gain
Printable HeartHealthy Checklist (downloadable)
At the end of this article youll find a simple PDF you can print and stick on your fridge. It includes daily medication reminders, a oneweek meal plan, and a quickexercise guide. Having it in plain sight turns good intentions into habits.
How to Talk to Your Doctor (empowering you)
Key questions to ask
Never feel intimidatedyour doctor is your partner. Here are some starter questions:
- What is the most appropriate acute treatment for my clot right now?
- What are the chances of another clot, and how can we lower that risk?
- Which medications do I need to take longterm, and what side effects should I watch for?
- Do I need any genetic testing for clotting disorders?
Understanding your test results
When you get an angiogram, youll see a series of images showing the narrowed segments. Ask the cardiologist to point out the culprit lesion and explain what they plan to do about it. Blood work that includes a platelet function test, lipid panel, and possibly a clotting factor screen can shed light on hidden risks.
Getting a second opinion
If a treatment plan feels rushed or you simply want reassurance, seeking another cardiologist is perfectly reasonable. Most hospitals make it easy to share your records electronically. A fresh set of eyes might suggest a different stent type or a slightly longer course of anticoagulationnothing harms a wellinformed patient.
Conclusion
Facing a coronary artery thrombosis is undeniably frightening, but knowing what works now and what lies ahead turns anxiety into action. Quick clotbusting therapy or a precise angioplasty can save heart muscle, while lifelong medicines and heartsmart habits keep the damage from returning. Remember, the best outcomes come from a blend of speedy medical care and steady, everyday choices.
If you or someone you care about is dealing with a clot, act fast, ask the right questions, and lean on trusted professionals. And dont forget to grab the printable checklist at the bottomsmall steps today lead to a stronger, healthier heart tomorrow.
FAQs
What is the fastest way to treat a coronary artery thrombosis?
Thrombolytic therapy (clot-busting medication) works fastest when administered within 3-6 hours of symptom onset, dissolving the clot chemically[2][8]. However, percutaneous coronary intervention (PCI) with angioplasty and stent placement is the preferred treatment at specialized centers, with guidelines recommending intervention within 90 minutes for high-risk patients to improve survival rates[1][3][7].
What medications are prescribed after coronary thrombosis treatment?
Long-term medication typically includes antiplatelet agents (aspirin and P2Y12 inhibitors like clopidogrel), anticoagulants for high-risk patients, statins to lower cholesterol, beta-blockers, and ACE inhibitors or ARBs to manage blood pressure and protect heart function[3][4][10]. Adherence to these medications is essential for preventing recurrent clots.
When is coronary artery bypass surgery (CABG) recommended?
CABG is recommended when multiple arteries are blocked or the anatomy is too complex for angioplasty and stent placement[1][5][7]. Surgeons graft a vein (typically from the leg) or artery from the chest to bypass blocked sections, providing complete revascularization though requiring longer recovery (approximately 6 weeks of rehabilitation).
What is the survival rate after coronary artery thrombosis?
Modern treatment achieves approximately 92% one-year survival rates when intervention occurs within the first six hours of symptom onset, with five-year survival around 80% for patients who maintain medication adherence and adopt heart-healthy lifestyle habits[1][2][7].
What are the main risks and side effects of coronary thrombosis treatment?
Anticoagulants increase bleeding risk (unexplained bruises, black stools, bleeding gums), while stents carry risks of restenosis (5-10% of cases) and late stent thrombosis if dual antiplatelet therapy is discontinued early[1][2]. Post-procedure complications may include arrhythmias and, in severe cases, heart failure requiring close medical follow-up.