Most people dont realize that the central nervous system can be silently invaded when someone is diagnosed with acute lymphoblastic leukemia (ALL). In fact, up to10% of adults already have CNS disease at the moment the blood test comes back positive.
Knowing the warning signs, how doctors look for it, and what the latest therapies are can mean the difference between a cure and a relapse. Lets break it down in plaintalk so you can understand whats really going on.
How common is it
What do recent studies tell us about prevalence?
Large multicenter analyses consistently report CNS involvement in ALL at diagnosis in roughly411% of patients. A 2022 review of over 3,000 adult cases found a median prevalence of7%, with higher rates in Tcell lineage disease. These numbers may feel small, but when you consider how aggressive CNS disease can be, theyre far from negligible.
Which subtypes carry the most risk?
When you dig into the data, a pattern emerges.
Agerelated differences
Pediatric patients historically have higher CNS ratesup to15% in some seriespartly because their bloodbrain barrier is more permissive. Adults, on the other hand, show a steadier 510% range. The takeaway? Regardless of age, the possibility of central nervous system involvement should never be dismissed.
| Group | Prevalence of CNS involvement |
|---|---|
| Pediatric ALL | 1215% |
| Adult Bcell ALL | 68% |
| Adult Tcell ALL | 912% |
Spotting key symptoms
Classic neurological red flags
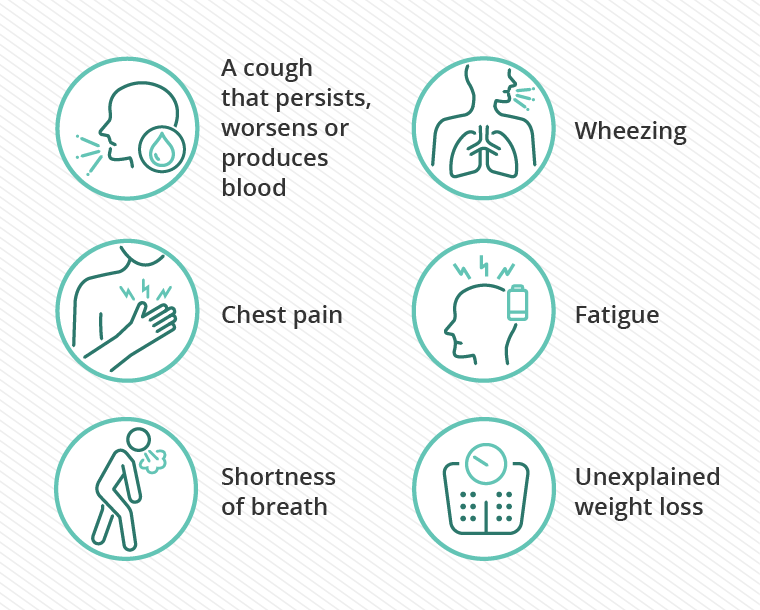
When leukemia spreads to the brain or spinal cord, the body often sends an SOS. Headaches that wake you at night, double vision, facial weakness, or sudden seizures are the loudest alarms. If you or someone you love experiences any of these, its time to call the oncology team immediately.
Subtle or messy presentations
Not every patient gets a dramatic seizure. Some report vague fatigue, subtle changes in mood, or difficulty concentratingsymptoms that could easily be blamed on chemotherapy itself. This messy picture is why many physicians stress the importance of routine cns all screening, even when nothing feels wrong.
Linking symptoms to lab clues
High whitecell counts, especially with blasts that express CD10 or CD34, raise suspicion. When a lumbar puncture later reveals blasts in the cerebrospinal fluid (CSF), the diagnosis of leukemia cns involvement becomes crystal clear. Remember, a normal blood count does NOT guarantee the CNS is clean.
Key diagnosis steps
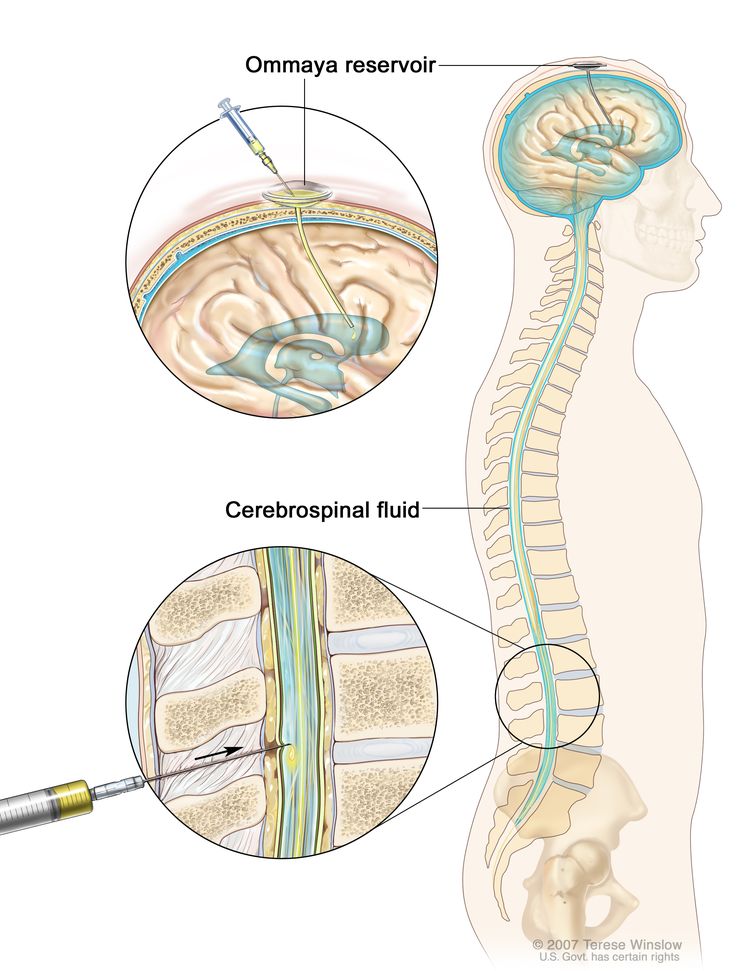
Standard workup: lumbar puncture
The cornerstone of detection is a careful lumbar puncture. Experts recommend a doubletap techniquecollecting fluid, then waiting a few minutes before a second drawto boost the chance of catching rare blasts. Cytology under the microscope is the first look, while flow cytometry adds a highresolution fingerprint of the cells.
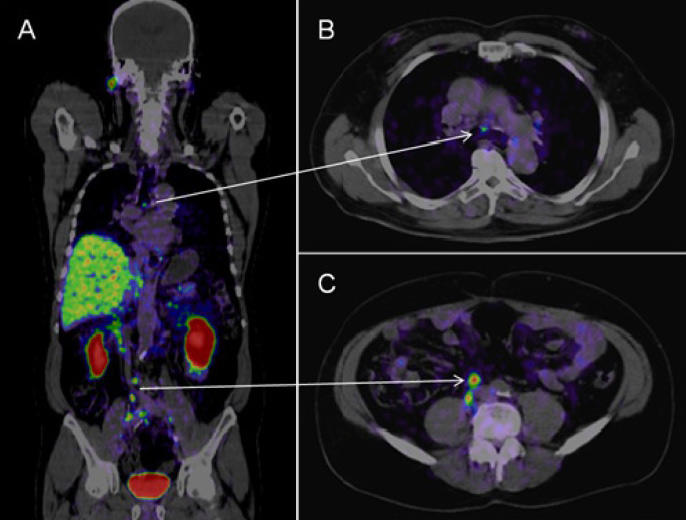
Imaging: when MRI adds value
Magnetic resonance imaging of the brain and spine isnt routine for every ALL patient, but it becomes essential when neurological symptoms appear or when CSF studies are inconclusive. MRI can reveal leptomeningeal enhancement, a telltale sign of meningitislike spread.
Emerging diagnostics
Nextgeneration sequencing (NGS) of CSF is an exciting frontier. A 2023 pilot study showed that NGS could detect leukemiaspecific mutations in CSF even when traditional cytology came back negative. , this approach may soon become a new standard for highrisk patients.
Effective treatment options
CNSdirected chemotherapy
Intrathecal (IT) therapydelivering drugs straight into the CSFremains the backbone of treatment. Methotrexate, cytarabine, and corticosteroids are the usual trio. Typical regimens involve 46 IT injections during induction, followed by maintenance doses every 46 weeks.
Systemic highdose regimens & targeted agents
Highdose systemic methotrexate can cross the bloodbrain barrier, offering an extra layer of protection. In recent years, monoclonal antibodies like blinatumomab and antibodydrug conjugates such as inotuzumab have shown CNS activity, especially in bcell all cns involvement cases. Clinical trials report remission rates of 7080% when these agents are combined with standard IT therapy.
Consolidation & maintenance: the role of radiation
Historically, cranial irradiation was the goto consolidation for CNSpositive ALL, but its longterm neurocognitive side effects have prompted a shift. Nowadays, many centers reserve radiation for refractory disease, opting instead for intensified chemotherapy schedules.
Clinical trial landscape (20242025)
CART cell therapy is making waves beyond the blood. Early phase trials show promising activity against CNS disease, with some patients achieving CSFnegative status after a single infusion. If youre exploring options, ask your oncologist whether a trial is appropriate for you.
Overall prognosis outlook
Survival rates & remission durability
Unfortunately, CNS involvement still dents overall outcomes. The cns leukemia survival rate for patients who clear CSF after induction hovers around 4555% at five years, compared with roughly 70% for those who never had CNS disease. That gap narrows when treatment is started early and when the disease is Bcell rather than Tcell.
Factors that improve outcomes
- Early detection (routine lumbar puncture at diagnosis)
- Achieving CSF negativity after induction
- Use of targeted agents in Bcell disease
- Enrollment in clinical trials
Longterm neurocognitive sequelae
Even when the leukemia is conquered, the CNS can bear scars. Survivors often report mild memory lapses, slowed processing speed, or occasional headaches. Regular neurocognitive screening, physiotherapy, and counseling can mitigate these effects and improve quality of life.
Real world stories
Patient vignette: a 34yearolds journey
James (name changed) was diagnosed with Bcell ALL after routine blood work. A few weeks into induction he complained of a persistent throbbing headache. A quick lumbar puncture revealed blastsclassic cns involvement in all. He received an intensive IT regimen, plus blinatumomab, and achieved CSF negativity after the third IT dose. Today, two years later, hes back at work, still attending regular neurological checkups but feeling hopeful.
Clinician insight
Dr. Patel, a hematologyoncology specialist with 15years of experience, says, We test every adult ALL patient at diagnosis because the stakes are high. Missing CNS disease is the biggest error we can make, and early IT therapy can turn a potentially fatal scenario into a curable one.
Caregiver FAQ excerpt
Q: Can my child develop CNS disease later if the initial CSF was clean?
A: Yes, it can. Thats why ongoing surveillancerepeat lumbar punctures during treatmentis standard practice.
Balancing benefits and risks
Benefits of aggressive CNS therapy
When you combine timely IT chemotherapy with systemic highdose agents, the chance of lasting remission jumps dramatically. In many cases, patients who would have relapsed in the CNS instead enjoy diseasefree survival beyond five years.
Risks & sideeffects to watch
Every treatment carries tradeoffs. Intrathecal methotrexate can cause chemical meningitis, manifested as fever and neck stiffness after the injection. Highdose systemic methotrexate may lead to kidney strain, requiring diligent hydration. And, as mentioned, cranial irradiationwhen usedcan affect memory and hormone production.
Shared decisionmaking checklist
Before you sign the treatment plan, consider asking:
- What is the goal of each CNSdirected therapy?
- How will my sideeffects be monitored and managed?
- Are there clinical trials that fit my profile?
- What longterm followup will I need for neurocognitive health?
Having these answers in hand turns a scary medical journey into a partnership you can navigate together.
Conclusion
CNS involvement in ALL isnt a rare footnoteits a critical factor that shapes diagnosis, treatment, and survival. Early recognition of all cns involvement symptoms, thorough lumbar puncture workup, and the use of modern intrathecal and targeted therapies can dramatically improve outcomes. At the same time, the benefits come with real risks that demand honest discussion and vigilant monitoring. If you or a loved one are walking this path, ask your doctor about CNS screening right away, explore clinicaltrial options, and stay alert for any neurological changes. Knowledge and partnership are the strongest weapons we have in this fight. For patients concerned about long-term outlook after major interventions, resources on prostate cancer outlook and survivorship can offer additional perspective on survivorship planning across cancers.
FAQs
What percentage of ALL patients have CNS involvement at diagnosis?
Approximately 4-11% of ALL patients show central nervous system involvement at diagnosis, with adults averaging around 7%, and higher rates in T-cell ALL subtype.
What are common symptoms indicating CNS involvement in ALL?
Key neurological symptoms include persistent headaches, double vision, facial weakness, seizures, and subtle signs like fatigue or concentration difficulties.
How is CNS involvement in ALL diagnosed?
Diagnosis primarily relies on lumbar puncture with cytology and flow cytometry of cerebrospinal fluid, supplemented by MRI when symptoms or CSF tests are inconclusive.
What treatments target CNS involvement in ALL?
Treatment includes intrathecal chemotherapy with methotrexate, cytarabine, corticosteroids, systemic high-dose methotrexate, and targeted agents like blinatumomab; radiation is now reserved for refractory cases.
Does CNS involvement affect the prognosis of ALL patients?
Yes, CNS involvement at diagnosis typically lowers survival rates (around 45-55% at five years) compared to those without CNS disease, but early detection and therapy improve outcomes.