We'll walk through the core drug classes, spotlight the latest breakthroughs, point out the top 10 kidneytoxic meds, and give you a practical stagebystage guide. By the end, you'll feel more confident about the choices you make for your kidneys and your health.
Core Drug Classes
ACE Inhibitors & ARBs
These two familiesACE inhibitors (like lisinopril and ramipril) and ARBs (such as losartan and irbesartan)are the cornerstone of chronic kidney disease medication. They lower blood pressure and, more importantly, reduce protein loss in the urine, a key marker of kidney damage.
Typical starting doses are low (e.g., lisinopril 5mg daily) and are slowly titrated up while monitoring potassium and creatinine. Sideeffects can include a persistent cough (ACEIs) or occasional dizziness. For many patients, these drugs are the best medicine for kidney disease recommended in the .
SGLT2 Inhibitors
Originally diabetes pills, SGLT2 inhibitors have turned into kidney protectors. Dapagliflozin (Farxiga) and empagliflozin (Jardiance) have shown in large trials (e.g., DAPACKD, EMPAKD) that they can slow eGFR decline by up to 30% compared with placebo.
Even if you're not diabetic, your doctor may prescribe a low doseoften 10mg daily. Watch for mild genital yeast infections, but overall the benefits far outweigh the risks for most CKD patients.
Calcium & Phosphate Binders
When kidneys can't clear phosphate, blood levels rise, leading to bone disease and vascular calcification. Binders such as calcium acetate, sevelamer, and lanthanum carbonate grab excess phosphate in the gut.
They're taken with meals; the usual dose is 1g3g three times a day, adjusted to keep serum phosphate in the target range. Sideeffects can include constipation (calcium agents) or bloating (sevelamer).
VitaminD Analogs & Calcimimetics
Kidney disease often triggers low active vitaminD and secondary hyperparathyroidism. Calcitriol, paricalcitol, and the calcimimetic cinacalcet help keep parathyroid hormone (PTH) levels in check, protecting bone health.
These are usually prescribed once daily, with dosage guided by calcium, phosphate, and PTH labs. Their role is especially crucial in stages 45 and for patients on dialysis.
Diuretics & BloodPressure Tweakers
Loop diuretics (e.g., furosemide) and thiazides (e.g., hydrochlorothiazide) manage fluid overloada common CKD symptom. Loop diuretics are stronger and often required in later stages, while thiazides work well early on when kidney function is still decent.
Monitoring electrolytes is vital; too much diuresis can worsen kidney function, so keep a weekly check on potassium and magnesium.
New Emerging Therapies
Finerenone
Finerenone is a nonsteroidal mineralocorticoid receptor antagonist approved in 2024 for patients with CKD and albuminuria. Compared with older drugs like spironolactone, it causes fewer potassium spikes while still offering heartandkidney protection.
Novel SGLT2 Combinations
Pharmaceuticals are now trialing fixeddose combos that pair an SGLT2 inhibitor with an ACEI or ARB, simplifying regimens and improving adherence. Early results suggest a smoother eGFR trajectory than using each drug separately.
RNABased Therapies
For rare forms of kidney disease (e.g., polycystic kidney disease), antisense oligonucleotides are entering PhaseII trials. Though still experimental, they represent a bold step toward targeting the disease at the genetic level.
Repurposed Drugs Patiromer
High potassium often forces clinicians to cut back on ACEIs/ARBs. Patiromer binds potassium in the gut, allowing patients to stay on their kidneyprotective meds without dangerous hyperkalaemia.
KidneyHarming Medications
| Drug Class | Common Examples | Why It Hurts Kidneys |
|---|---|---|
| Nonsteroidal antiinflammatory drugs (NSAIDs) | Ibuprofen, Naproxen, Diclofenac | Reduce blood flow to nephrons, causing acute tubular necrosis. |
| Aminoglycoside Antibiotics | Gentamicin, Tobramycin | Direct tubular toxicity; requires serum level monitoring. |
| Contrast Imaging Agents | Iodinated contrast, Gadolinium | Can trigger contrastinduced nephropathy; hydration helps mitigate risk. |
| ProtonPump Inhibitors (Longterm) | Omeprazole, Esomeprazole | Metaanalyses link chronic use to CKD progression. |
| Herbal Supplements (Nephrotoxic) | Aristolochic acid, certain Chinese herbs | Direct renal cortex damage; often unregulated. |
| HighDose Diuretics | Furosemide >80mg/day | Excessive volume depletion can impair renal perfusion. |
| Statins (Rarely) | Atorvastatin high dose | Rare myopathy leading to rhabdomyolysis, straining kidneys. |
| Calcineurin Inhibitors | Cyclosporine, Tacrolimus | Nephrotoxic effect via vasoconstriction; used cautiously in transplant. |
| Antiretrovirals (Certain) | Tenofovir disoproxil fumarate | Can cause proximal tubular dysfunction. |
| NSAIDContaining Topicals | Diclofenac gel | Even topical forms can be absorbed and affect kidneys. |
Understanding this top 10 drugs that cause kidney damage list helps you spot red flags on prescription bottles and overthecounter shelves. If you're ever unsure, a quick chat with your pharmacist can save you a lot of worry.
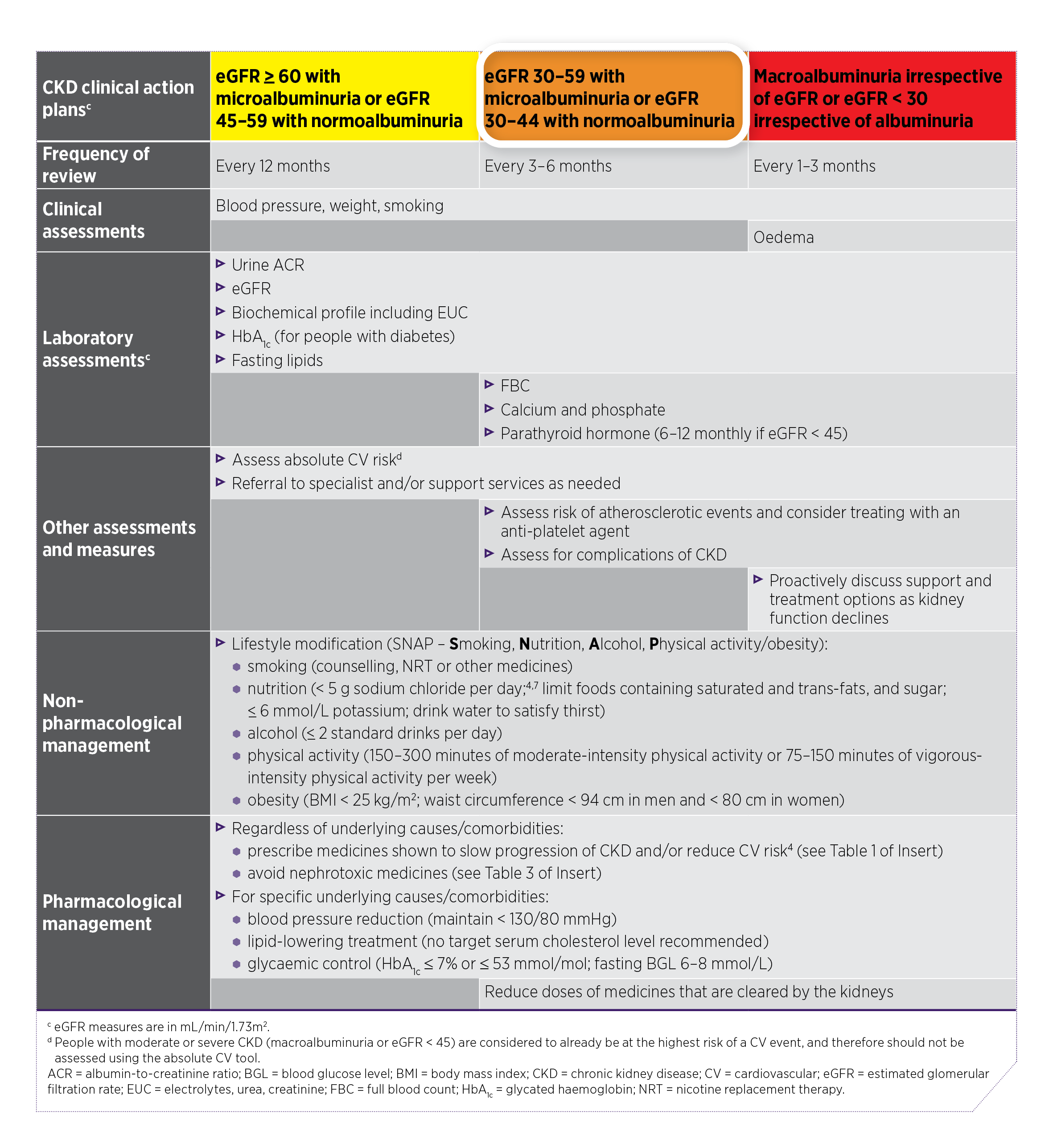
StageBased Medication Guide
Early CKD (Stages 12)
Goal: Slow progression, control blood pressure, and start lifestyle changes. ACEI or ARB is usually the first prescription, often paired with a lowdose statin for cardiovascular protection.
Moderate CKD (Stages 34)
Beyond blood pressure, you'll likely add an SGLT2 inhibitor and maybe a phosphate binder if labs show high phosphate. VitaminD analogs become important if PTH rises.
Advanced CKD (Stage 5 / Dialysis)
Dosing changes: many drugs need reduction or avoidance. For example, metformin is usually stopped, and erythropoiesisstimulating agents may be added to manage anemia. Keep a medication list handy for your dialysis team. For patients and caregivers looking for practical cost information about some newer agents, resources on drug pricing can be helpful when discussing options with your team; checking current details such as Lokelma cost may clarify access and affordability when patiromer or other newer agents are considered.
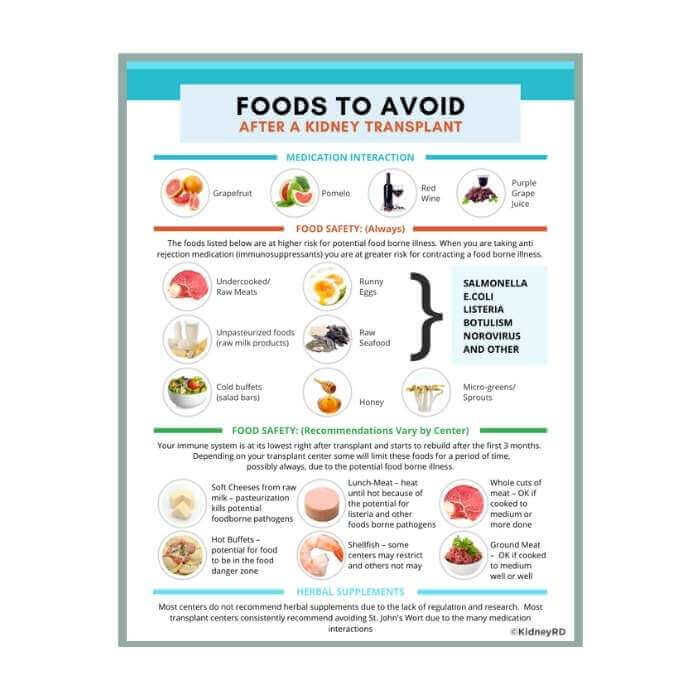
PostTransplant Care
Immunosuppressants (tacrolimus, mycophenolate) are essential, but they come with their own kidneyrisk profile. Close monitoring and a kidneyfriendly adjunct like a lowdose ACEI can help protect the new graft.
Balancing Benefits & Risks
RiskBenefit Scoring Sheet
Consider creating a simple table (your doctor can help) that lists each medication, its primary benefit for CKD, and potential sideeffects. Score each on a 15 scale; the higher the benefit and the lower the risk, the more likely it is a good fit.
When to Ask for a Medication Review
If you notice any of the following, it's time for a chat with your nephrologist:
- Sudden rise in creatinine or drop in eGFR.
- Persistent swelling, shortness of breath, or unusual fatigue.
- New skin rashes or frequent infections.
- Any pill fatigue feeling overwhelmed by the number of tablets.
Lab Monitoring Checklist
Regular labs are the compass that tells you whether a medication is helping or hurting:
- eGFR & Creatinine: Every 36 months (more often if meds change).
- Potassium: ACEI/ARB, SGLT2, and finerenone can raise levels.
- Phosphate & Calcium: Important when using binders or vitaminD analogs.
- Urine Albumin: Tracks protein lossaim for the lowest possible.
All of this data helps you and your clinician make informed decisions, keeping the balance between protecting kidneys and maintaining quality of life.
Helpful Resources
For deeper dives, the following sites offer evidencebased guidance:
- Recent peerreviewed articles (20232025) on finerenone, SGLT2 inhibitors, and RNA therapies (search PubMed for finerenone CKD 2024).
Final Takeaways
Knowing the CKD medication list isn't just about memorizing drug names; it's about understanding why each pill is there, what it hopes to accomplish, and where the pitfalls lie. From ACEIs and SGLT2 inhibitors that truly protect kidney function, to the sneaky overthecounter culprits that can silently damage them, the picture becomes clearer when we look at both sides of the coin.
Remember, every person's journey with chronic kidney disease is unique. Use this guide as a conversation starter with your healthcare team, not as a replacement for professional advice. If you have questions, share your thoughts in the comments, download the printable checklist, or set up a medicationreview appointment. Your kidneys deserve that attention, and you deserve peace of mind.
FAQs
What are the main medications used for CKD?
ACE inhibitors, ARBs, SGLT2 inhibitors, phosphate binders, vitamin D analogs, and diuretics are commonly prescribed for CKD.
Are there new medications for CKD?
Yes, finerenone and new SGLT2 inhibitor combinations are recent additions to CKD treatment options.
Which drugs should be avoided with CKD?
NSAIDs, aminoglycoside antibiotics, certain antivirals, and some herbal supplements can harm kidneys and should be avoided.
Do CKD medications need dose adjustments?
Yes, many CKD medications require dose adjustments based on kidney function to prevent side effects.
Can over-the-counter painkillers affect CKD?
Yes, NSAIDs like ibuprofen can worsen CKD and should be avoided unless approved by a doctor.
What is the role of SGLT2 inhibitors in CKD?
SGLT2 inhibitors slow CKD progression and reduce cardiovascular risk, even in non-diabetic patients.
How often should CKD medications be reviewed?
CKD medications should be reviewed regularly, especially if kidney function changes or new symptoms appear.