Most people dont realize that catching a sarcoma early can change everything for a childs health. In a nutshell, a childhood sarcoma diagnosis means a doctor has confirmedusually with imaging and a biopsythat a malignant tumor has formed in the bone or soft tissue of your child. The process can feel overwhelming, but knowing the exact steps, the warning signs, and what comes after the diagnosis can give you the power to act quickly and confidently.
In the next few minutes, Ill walk you through what sarcoma looks like in kids, how doctors pinpoint it, the different types you might hear about, and what the survival numbers really mean. Think of this as a friendly chat over coffeeno jargon, just clear answers you can use right now.
Understanding Childhood Sarcoma
Sarcoma is a broad term for cancers that start in connective tissueslike bone, muscle, fat, cartilage, or blood vessels. In children, these tumors are rare but serious, and they behave differently from adult sarcomas. The most common malignant softtissue tumors in kids include rhabdomyosarcoma and Ewing sarcoma, while the most common benign soft tissue tumor in childhood is usually a hemangioma.
According to the National Cancer Institutes PDQ, bone sarcomas make up about 3% of all childhood cancers, whereas softtissue sarcomas account for roughly 7%. While the numbers sound small, every case is a deeply personal story for families.
How common are sarcomas in kids?
| Age Group | Incidence (per 1M) | Typical Types |
|---|---|---|
| 04 years | 5 | Rhabdomyosarcoma, Embryonal |
| 514 years | 12 | Ewing sarcoma, Alveolar rhabdomyosarcoma |
| 1519 years | 7 | Bone sarcoma, Synovial sarcoma |
Why a biopsy matters
If youve ever Googled sarcoma child symptoms, youll quickly see that many signslike a painless lumpoverlap with harmless conditions. The only way doctors can be certain its a sarcoma is through a tissue sample, often called a core needle or open biopsy. , a biopsy not only confirms malignancy but also tells the lab which genetic markers are present, shaping the treatment plan.
Spotting Sarcoma Symptoms
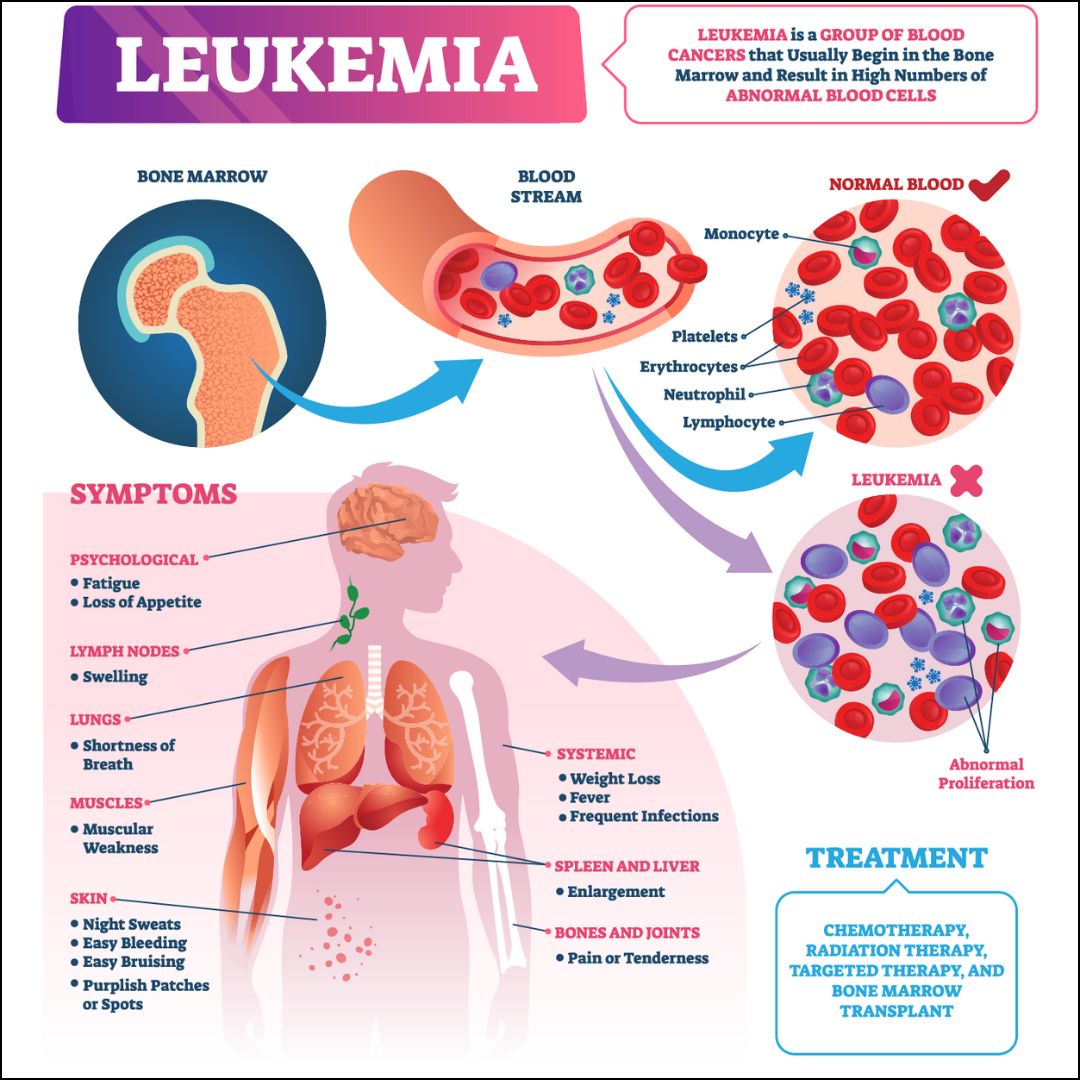
Remember the last time you felt a knot in your thigh and just brushed it off? For many parents, thats the first clueonly that the knot might be a tumor growing silently. Children with cancers such as sarcoma or leukemia may also display systemic symptoms like unexplained fever, weight loss, or fatigue, which sometimes overlap with warning signs seen in leukemia pregnancy treatment cases, though the underlying causes and typical ages differ.
Typical warning signs
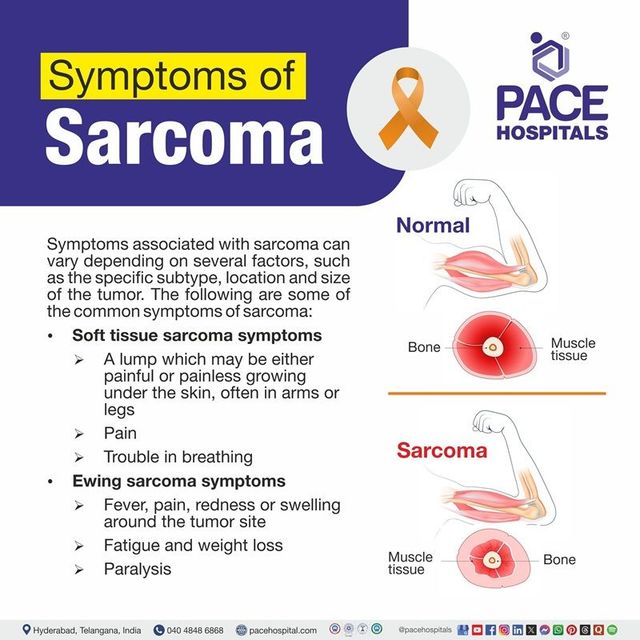
- Painless, firm lump that doesnt go away
- Swelling that gets bigger over weeks
- Night pain that wakes your child
- Limited movement in a limb
- Unexplained fever, weight loss, or fatigue
When to act fast
If the lump is rapidly enlarging, changes color, or is accompanied by fever, its a redflag that needs urgent evaluation. A simple checklist can help you remember:
- Is the lump >1cm?
- Does it feel hard or firm?
- Is it getting bigger?
- Does your child complain of pain at night?
Diagnostic Steps Explained
Getting a diagnosis isnt a single test; its a journey that starts with a conversation and ends with a clear treatment roadmap.
First medical visit
Doctors will ask about the lumps history, your childs overall health, and any family cancer history. A thorough physical exam follows, often including measurements and a quick look at your childs mobility.
Imaging studies
Imaging helps map the tumors size, location, and relationship to nearby structures. Common modalities include:
- Xray: First look, especially for bone involvement.
- Ultrasound: Good for superficial softtissue lumps.
- MRI: The gold standard for defining softtissue sarcoma in children.
- CT scan: Helpful for chest evaluationchecking if the cancer has spread.
- PET scan: Highlights metabolic activity, useful in staging.
Biopsy the definitive test
There are three main biopsy techniques:
- Core needle biopsy: A thin needle extracts a tissue core; minimally invasive.
- Open (incisional) biopsy: A small incision lets surgeons take a larger piece.
- Excisional biopsy: The entire lump is removedusually if its small and appears benign.
Choosing the right method depends on the tumors location and size. A study from the National Cancer Institute shows that core needle biopsies achieve accurate diagnoses in over 90% of pediatric sarcoma cases, while keeping complications low.
Pathology review
Once the tissue reaches the lab, a pediatric soft tissue tumors pathology expert stains the sample, looks for characteristic cell shapes, and runs genetic tests. The resulting report includes:
- Histologic type (e.g., rhabdomyosarcoma)
- Grade (how aggressive the cells look)
- Margins (whether cancer cells are at the edge of the sample)
- Molecular markers (like PAXFOXO1 fusion in alveolar rhabdomyosarcoma)
Sarcoma Types That Matter
Not all sarcomas are created equal. Knowing the main families helps you understand prognosis and treatment options.
Softtissue versus bone sarcoma
Softtissue sarcomas arise in muscles, fat, nerves, or blood vessels, while bone sarcomas start in the marrow or cortex of bone. Both can spread (metastasize), but they often respond to different chemotherapy regimens.
Common malignant types
| Type | Typical Age | Key Features | 5Year Survival |
|---|---|---|---|
| Rhabdomyosarcoma | 014 yrs | Musclederived, often in head/neck or genitourinary tract | 70% (localized) |
| Ewing Sarcoma | 1020 yrs | Bone/softtissue, translocation t(11;22) | 65% (localized) |
| Synovial Sarcoma | 1530 yrs | Often near joints, SS18-SSX fusion | 55% (localized) |
Benign lookalikes
Even benign tumors can mimic sarcoma on imaging. For instance, a large hemangioma (the most common benign soft tissue tumor in childhood) may appear suspicious on an MRI, prompting a biopsy to rule out malignancy.
Interpreting Test Results
After the pathology report, the next step is stagingfiguring out how far the cancer has spread.
Staging basics
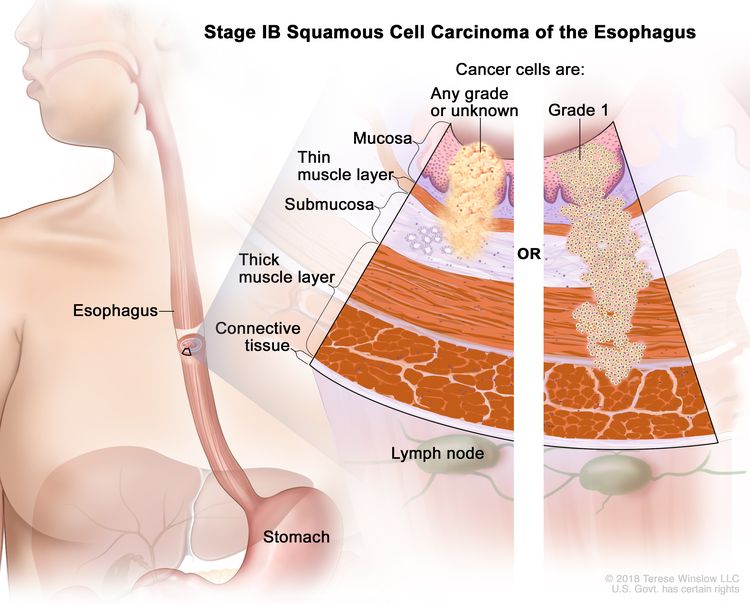
- Stage I: Localized, small tumor.
- Stage II: Larger but still confined.
- Stage III: Involves regional lymph nodes.
- Stage IV: Distant metastasis (often lungs).
Molecular and genetic testing
Many modern sarcoma protocols include nextgeneration sequencing to detect mutations that open doors to targeted therapies. For example, infants with an ALKpositive rhabdomyosarcoma may qualify for ALK inhibitors, a breakthrough highlighted in the . In some cancers, such as those affecting the prostate, genetics can play a significant role; see more on colon cancer genetic testing and its parallels to genetic testing approaches in sarcoma diagnosis.
Multidisciplinary tumor board
Once staging is clear, a teampediatric oncologists, surgeons, radiologists, pathologists, and sometimes psychologistsconvenes to craft a personalized treatment plan. This collaborative approach ensures every angle, from surgical margins to emotional support, is covered.
Balancing Benefits and Risks
Every diagnostic step carries both upside and potential downsides. Understanding this balance can help you make informed decisions without panic.
Benefits of early diagnosis
- Higher chance of complete surgical removal
- Possibility of lowerdose chemotherapy
- Better overall survival rates
Potential risks
- Biopsy complications (bleeding, infection)
- Emotional stress for the child and family
- Falsepositive results, though rare, can cause unnecessary anxiety
Supporting your child emotionally
Kids sense our worries. Keeping a calm, honest toneexplaining that were doing the best tests to help the doctors find the right treatmentcan reduce fear. Consider involving a child psychologist or joining a support group like those offered by .
Survival Outlook
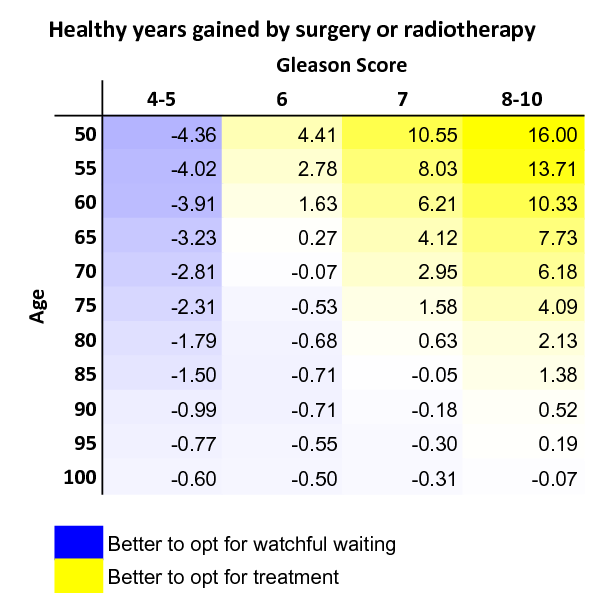
Numbers can feel cold, but they also give hope. The pediatric sarcoma survival rate varies widely by subtype, stage, and age. For comparison, in adult cancers, survival varies significantly by site and therapy: for example, adults undergoing prostate removal life expectancy is generally very favorable when detected early, just as with early-stage sarcomas in children.
Overall survival trends
- Localized softtissue sarcoma: ~7080% 5year survival.
- Localized bone sarcoma (e.g., Ewing): ~6570%.
- Metastatic disease: drops to 2030% in many cases.
Factors that improve odds
- Early-stage detection (the sooner, the better).
- Access to specialized pediatric oncology centers.
- Participation in clinical trials offering cuttingedge therapies.
What the statistics mean for you
Every childs story is unique. While statistics provide a backdrop, your childs response to treatment, the expertise of the care team, and the support network you build can tilt the odds in your favor.
Next Steps for Families
Now that youve got the roadmap, what should you do next?
Build your care team
Look for a pediatric oncology center with a dedicated sarcoma program. Hospitals like NYU Langone, MD Anderson, and Nationwide Childrens have multidisciplinary teams that specialize in these rare cancers.
Second opinions are okay
Its perfectly normal to seek a second opinionespecially before major surgery or intensive chemotherapy. Most top centers welcome referrals and can work together to guarantee the best care.
Financial and practical help
Many hospitals offer financial counselors who can navigate insurance, copays, and charitable assistance. Organizations such as the provide travel grants and lodging for families traveling long distances.
Stay connected
Join online communities or local support groups. Hearing other families stories can provide practical tips (like the best kidfriendly hospital snacks) and emotional comfort.
Conclusion
Getting a childhood sarcoma diagnosis is never easy, but knowing the exact stepsfrom spotting the first symptom to understanding biopsy resultsempowers you to act swiftly and confidently. Early, accurate diagnosis opens the door to tailored treatment, improves survival odds, and gives your child the best possible chance at a healthy future. Remember, youre not alone: a dedicated medical team, trusted resources, and a supportive community are all within reach. If you have questions or want to share your own journey, feel free to leave a comment belowlets keep the conversation going.
FAQs
What are the early signs of a childhood sarcoma?
Often a painless, firm lump that grows over weeks, night‑time pain, swelling, limited limb movement, or unexplained fever, weight loss, and fatigue.
How is a childhood sarcoma diagnosis confirmed?
Doctors first use imaging (X‑ray, MRI, CT, PET) to locate the tumor, then obtain a tissue sample through a core needle, open, or excisional biopsy for pathological and genetic analysis.
Which imaging tests are typically done before a biopsy?
Initial X‑ray or ultrasound may be followed by MRI for soft‑tissue detail, CT for chest evaluation, and sometimes PET scans to assess metabolic activity and possible spread.
What treatment options are available after the sarcoma is staged?
Depending on stage and type, treatment may include surgery to remove the tumor, chemotherapy, radiation therapy, targeted drugs for specific genetic markers, and enrollment in clinical trials.
How can families cope emotionally during the diagnosis process?
Maintain open, honest communication with age‑appropriate language, seek support from child psychologists, join pediatric cancer support groups, and use hospital social‑work services for practical help.