Got a diagnosis of cervical cancer and hear FIGO stage tossed around? It can feel like youve just been handed a secret code. In the next few minutes Im going to decode that code, show you what each stage really means, and explain why the newest 2024 updates matter for you or your loved one. No medical jargon, just clear, friendly answers so you can talk to your doctor with confidence.
Well walk through the staging chart, peek at the latest imaging tricks, and point out the biggest dos and donts of interpreting a FIGO stage. Think of it as a hearttoheart chat with a friend whos done the homework so you dont have to.
Quick Look Overview
What is FIGO?
FIGO stands for the International Federation of Gynecology and Obstetrics. Since the 1950s its been the global standard for describing how far cervical cancer has spread. While other systems like TNM exist, FIGO is the one most oncologists use when they tell you your cancer is stageIIA.
Why FIGO matters more than TNM
| Aspect | FIGO | TNM |
|---|---|---|
| Focus | Clinical exam + imaging | Anatomical size + nodal status |
| Global acceptance | Widely used in guidelines | More common in research studies |
| Treatment guidance | Directly linked to therapy choices | Often supplemental |
Source credibility
All the numbers below come from the and are echoed by the American Cancer Societys 2025 update on cervicalcancer staging.
Stage Details
Stage0 Carcinoma insitu
At this earliest point, abnormal cells are confined to the surface layer of the cervix. Its usually spotted during a routine Pap test, and treatment is often a simple loop electrosurgical excision procedure (LEEP). No imaging needed, just a quick pathology check.
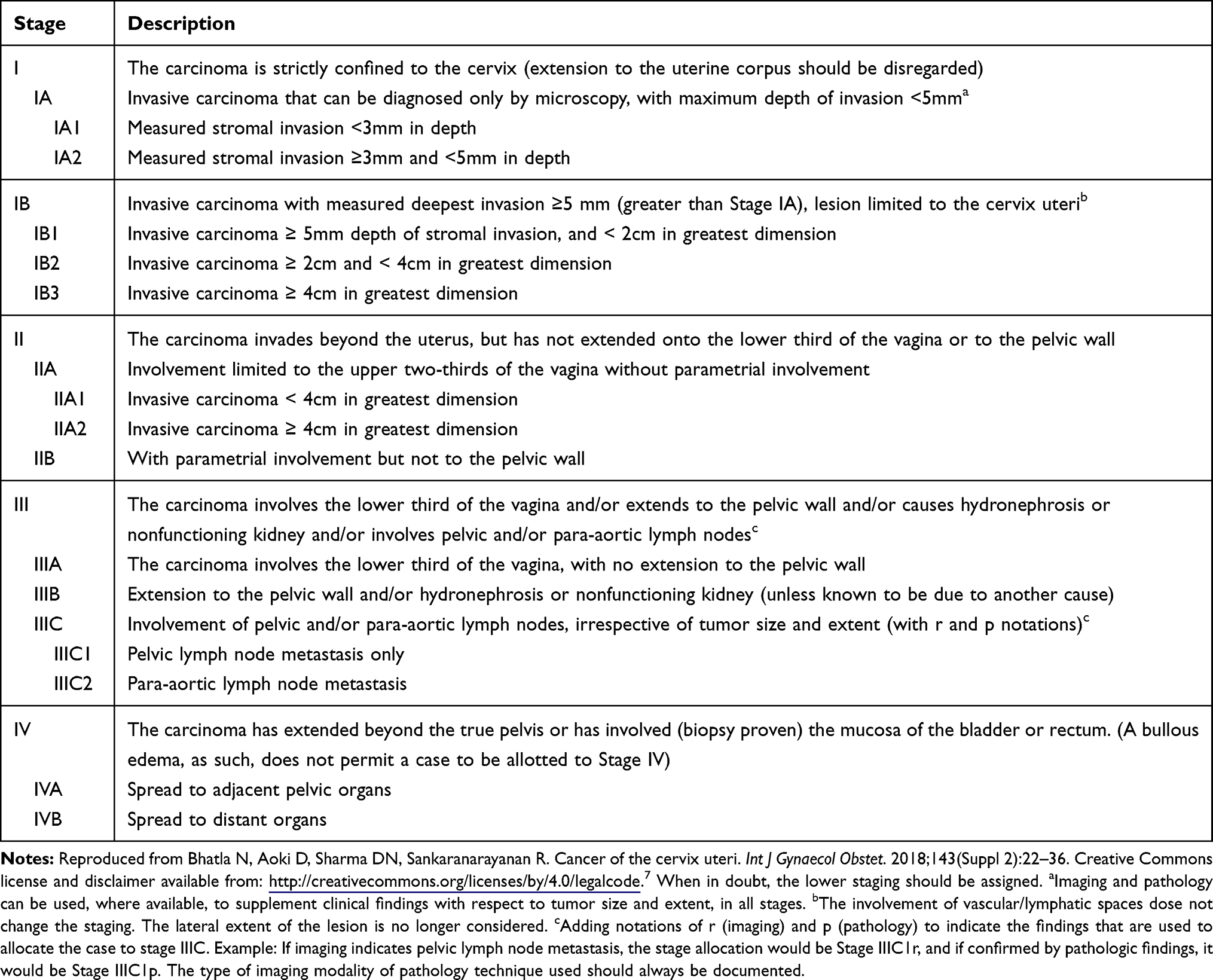
StageI Confined to the cervix
StageI is split into IA and IB. IA means the tumor is microscopic (visible only under a microscope), while IB covers visible tumors that havent reached beyond the cervix.
IA1 & IA2 (microinvasive)
IA1 tumors are 3mm deep and 7mm wide; IA2 are a bit larger (5mm deep). Because theyre tiny, most doctors recommend a cone biopsy or simple hysterectomy. A realworld example: Maria, a 32yearold mother of two, learned her IA2 tumor was removed with a fertilitypreserving cone shes now cancerfree and planning another baby.
IB1, IB2, IB3 (2024 update)
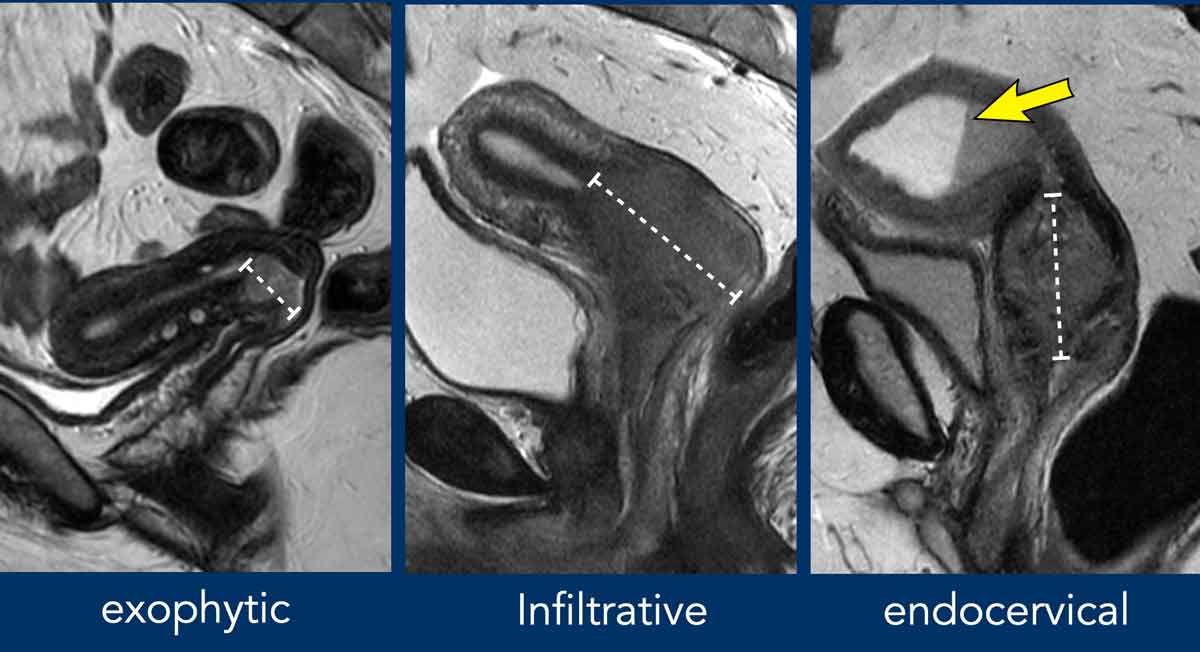
20232024 revisions introduced new size cutoffs: IB1 is <2cm, IB2 is 24cm, and IB3 is >4cm. The shift matters because it helps decide whether youll get surgery alone or need chemoradiation. MRI is the goto imaging tool for measuring these tumors accurately.
StageII Spread beyond the cervix but not to the pelvis sidewall
IIA means the cancer reached the upper vagina without parametrial invasion. IIB indicates parametrium involvement a trickier situation that often calls for combined chemoradiation.
Mnemonic for IIA vs IIB
Think IIAB = Above, Below. A (above) = upper vagina only; B (below) = parametrium.
StageIII Involvement of the lower vagina or pelvic lymph nodes
IIIA indicates the tumor has extended to the lower third of the vagina, while IIIB signals a push into the pelvic wall or causing hydronephrosis. The 2018 FIGO revision added the IIIC category for nodal disease:
- IIIC1 Positive pelvic lymph nodes
- IIIC2 Positive paraaortic nodes
Knowing whether nodes are involved changes the treatment plan dramatically often steering doctors toward extended field radiation.
StageIV Distant spread
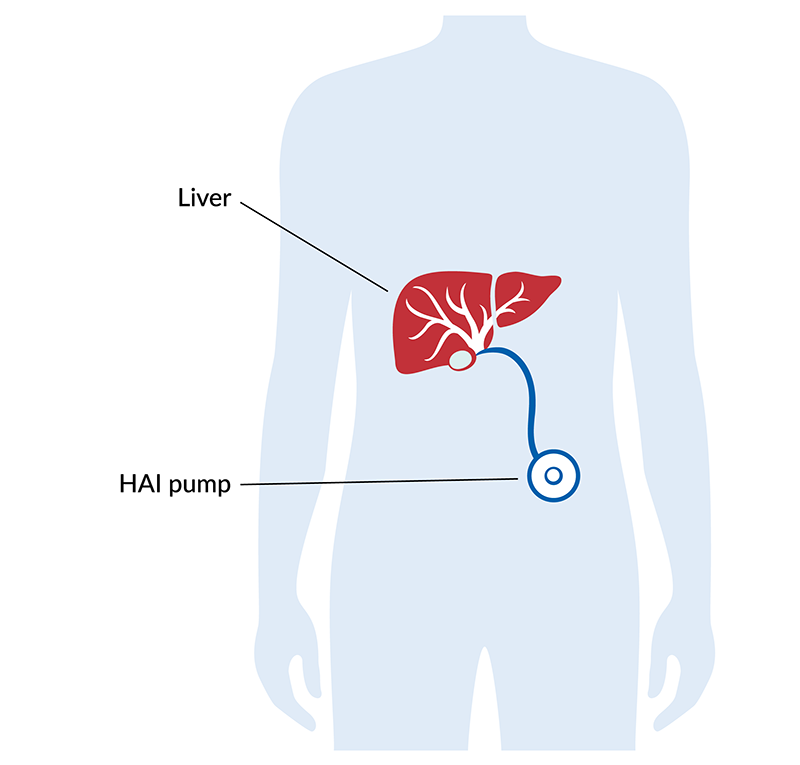
IVA means the cancer has invaded nearby organs such as the bladder or rectum. IVB is when its traveled to distant sites like the lungs or liver. PETCT is essential here for mapping the full picture, and treatment shifts toward palliative intent.
Latest Updates 2024
New size cutoffs
The 20232024 revision tightened the IB subcategories. Why? Studies showed that patients with tumors >4cm (now IB3) had poorer outcomes with surgery alone, so chemoradiation became the favored route.
Imaging upgrades
MRI is now mandatory for assessing parametrial invasion. A 2020 radiology study highlighted that MRIs softtissue contrast catches subtle spread that CT often misses, making staging more accurate.
Lymphnode classification (IIIC1 vs IIIC2)
Splitting nodal disease into pelvic (IIIC1) and paraaortic (IIIC2) helps predict survival. Patients with IIIC2 disease generally need a larger radiation field and sometimes upfront chemotherapy.
Quick PDF download
For a printable reference, grab the . Its a handy cheatsheet you can keep in your medical folder.
Reading Your Report
Decoding the terminology
| Abbreviation | What it means |
|---|---|
| LVSI | Lymphvascular space invasion cancer cells in tiny vessels |
| Parametrium | Connective tissue surrounding the cervix |
| Hernia | Not related just a typo many patients spot in reports! |
What to ask your oncologist
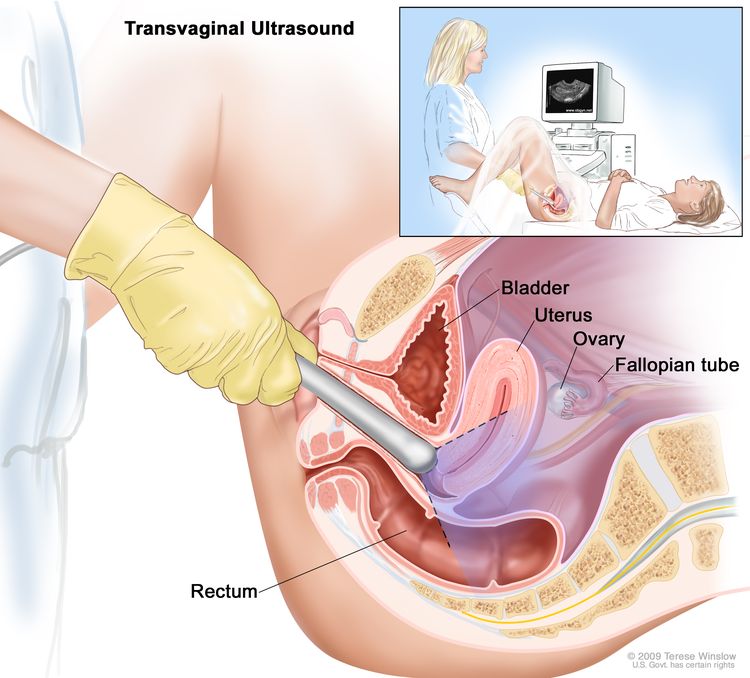
- Is the stage confirmed by imaging (MRI/CT/PET) or only clinical exam?
- Do we need additional tests to check lymph nodes?
- How does my specific stage guide treatment options?
- What are the chances of upstaging after surgery?
- Are there clinical trials that match my stage?
Common misunderstandings
Many think StageII means surgery is off the table. Not true some earlyIIA tumors are still surgically resectable, especially when the parametrium isnt involved. An OBGYN oncologist quoted in Obstetrics & Gynecology (2021) clarified that stage alone doesnt dictate surgery; tumor size, patient health, and fertility wishes all play a role.
Benefits & Risks
Benefits of accurate FIGO staging
When the stage is spoton, treatment can be precisely tailored, which can mean fewer side effects, higher cure rates, and eligibility for cuttingedge clinical trials. It also gives you a realistic picture of prognosis, helping you plan ahead.
Risks / Limitations
Staging isnt perfect. Interobserver variabilitydifferent doctors may read the same MRI differentlycan lead to under or overstaging. Imaging technology varies by center, so a community hospitals CT might miss small nodal disease that a tertiarycenter PETCT would catch. Overstaging can push patients into more aggressive therapy than needed, while understaging may leave hidden disease untreated.
Realworld case
Emma, a 45yearold from Ohio, was initially staged as IIB after an MRI. A subsequent PETCT revealed isolated pelvic nodes, bumping her to IIIC1. Because of that change, her team added a short course of chemotherapy before radiation, and shes now diseasefree two years later. Her story underscores why a second look can be a lifesaver.
Real World Examples
Case study: Fertilitypreserving option
Laura, age29, was diagnosed with stageIA2. She wanted to keep her chance of having children. Her surgeon performed a radical trachelectomya uterussparing operationfollowed by close surveillance. Five years later, Laura delivered a healthy baby. This illustrates how early FIGO stages can open doors to lessdrastic surgery.
Case study: When staging changes after surgery
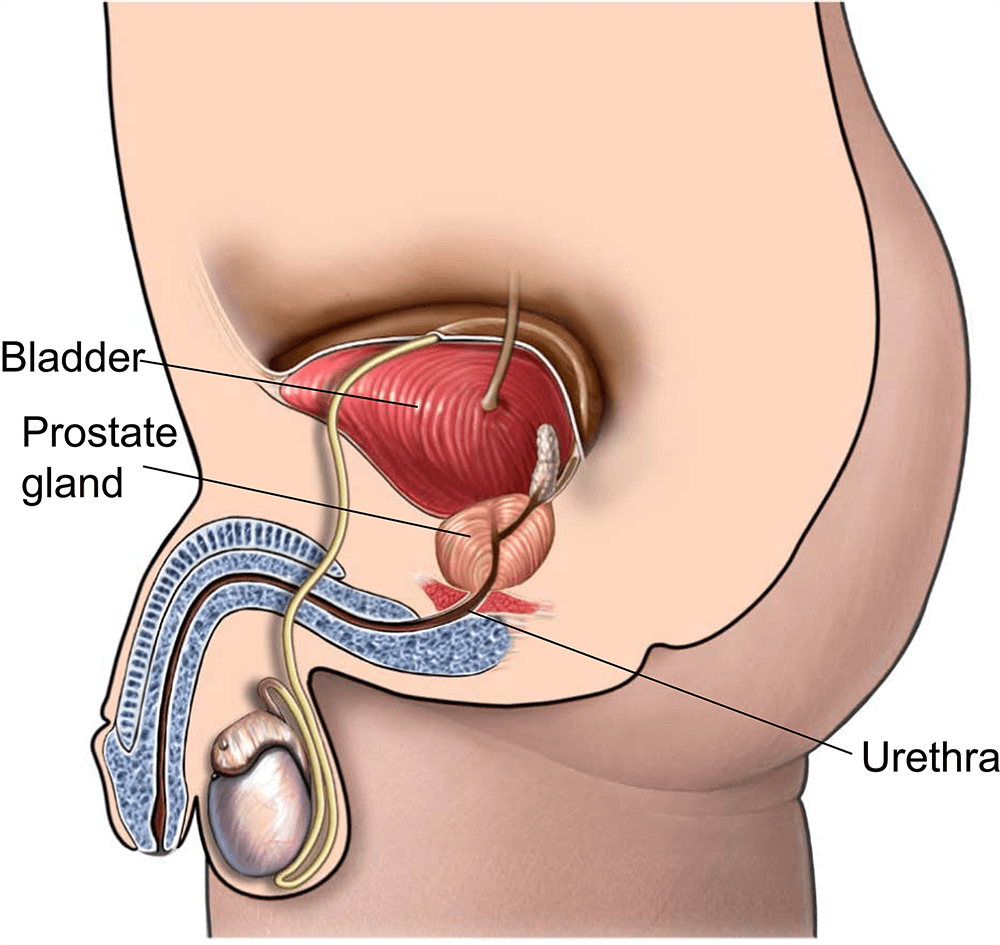
Mark, 52, had a tumor that looked like stageIB1 on MRI. After a simple hysterectomy, pathology showed microscopic spread to a pelvic node, reclassifying him as IIIC1. His oncologist recommended adjuvant chemoradiation, which he completed successfully. The lesson? Surgical pathology can sometimes reveal a higher stage, and thats why the FIGO system incorporates both clinical and pathological data. If youre reviewing longterm outlooks after surgery, resources on prostate cancer outlook can provide a useful comparison of how staging affects prognosis across cancers.
Putting It All Together
Understanding the cervical cancer staging FIGO system is the first step toward personalized care. The 2024 updatesnew tumorsize thresholds, mandatory MRI, and a refined nodal classificationgive doctors sharper tools, but they also bring new questions. By knowing what each stage truly means, what imaging to expect, and the right questions to ask, you can turn uncertainty into empowerment.
If you want a printable cheatsheet or deeper dive into treatment options, check the resources above and keep an open conversation with your care team. Knowledge is powerstay informed, stay proactive, and remember youre not alone on this journey.
FAQs
What does FIGO staging mean in cervical cancer?
FIGO staging is a global system used to describe how far cervical cancer has spread. It helps doctors determine treatment and prognosis based on clinical exam, imaging, and pathology findings.
What are the main changes in FIGO staging for cervical cancer in 2024?
The 2024 update introduced new tumor size cutoffs for stage IB subcategories, mandatory MRI for parametrial invasion assessment, and refined lymph node classifications dividing pelvic (IIIC1) and paraaortic (IIIC2) nodes.
How is stage IIIC different from earlier FIGO stages?
Stage IIIC specifically indicates lymph node involvement, subdivided into IIIC1 for pelvic nodes and IIIC2 for paraaortic nodes, significantly affecting prognosis and treatment planning.
Why is MRI important in the new FIGO staging system?
MRI offers superior soft-tissue contrast to detect subtle tumor spread and parametrial invasion, making staging more accurate and guiding better treatment decisions.
Can FIGO staging change after surgery?
Yes. Initial clinical staging can be updated based on surgical pathology results, such as detecting microscopic lymph node metastasis, which may upstage the cancer and alter treatment plans.