Hey there! If youve ever wondered why someone suddenly starts missing objects when they reach for them, or why they cant shift their gaze across a room, the answer often lies in Balints syndrome. In a nutshell, this puzzling condition pops up when the bilateral parietooccipital cortex gets hurt. Below, well walk through what that means, how it shows up in everyday life, and what you (or a loved one) can do about itall in a friendly, easytodigest style.
Quick Answer
Balints syndrome is associated with damage to the bilateral parietooccipital (posterior parietaltemporal) cortex. This damage throws a wrench into the brains visualspatial integration, producing the classic triad of symptoms: optic ataxia, ocular apraxia (or simultanagnosia), and impaired gaze shifting.
Why It Matters
Core Symptoms Youll Actually Feel
Imagine trying to pick up a coffee mug, but your hand keeps aiming for the empty space beside it. Thats optic ataxia. Or picture watching a movie and finding yourself stuck on a single corner of the screen, unable to take in the whole scenewelcome to ocular apraxia, also called simultanagnosia. When all three symptoms roll together, we call it the Balint syndrome triad. These arent just clinical buzzwords; they dramatically affect daily routines, from grocery shopping to driving.
Everyday Examples That Stick
- Grocerystore navigation: You reach for a carton of milk, but your hand grabs at the shelf instead.
- Reading a menu: You stare at a single item and cant scan the rest of the page.
- Crossing the street: Multiple cars appear, yet your eyes fixate on one, making it hard to notice the others.
MiniChecklist for Readers
| Symptom | Typical behavior | Quick selfscreen question |
|---|---|---|
| Optic ataxia | Misses objects when reaching | Do you often grab at empty air? |
| Ocular apraxia | Cannot scan a scene | Do you feel stuck on one point of view? |
| Simultanagnosia | Cant see more than one thing | Do you lose track if two things appear together? |
Anatomy Behind Damage
Which Brain Regions Are Involved?
The culprit is usually the bilateral parietaloccipital cortexthink of it as the brains backstage crew that coordinates where things are and how we move toward them. The precuneus, superior occipital gyri, and parts of the temporoparietal junction also join the party when the damage spreads.
Common Causes of That Damage
Not all brain injuries are created equal. Heres the usual suspects:
- Ischemic infarcts (stroke): Sudden loss of blood flow hits the posterior regions hardest. notes this as the most frequent cause.
- Traumatic brain injury: A blow to the head can bruise both sides of the posterior cortex.
- Neurodegenerative diseases: Conditions like Lewybody dementia can erode those same areas over time.
- Tumors, infections, severe migraines: Less common, but they can produce a similar pattern of damage.
Etiology vs. Typical MRI Findings
| Etiology | MRI pattern | Typical onset |
|---|---|---|
| Bilateral ischemic infarct | Symmetrical hyperintensities in parietooccipital white matter | Acutesubacute |
| Trauma (contusion) | Focal cortical bruising + edema | Hoursdays |
| Diffuse Lewybody disease | Cortical atrophy, especially posterior | Insidious |
| Tumor (glioma) | Mass effect & contrastenhancing lesions | Variable |
How Its Diagnosed
Clinical Bedside Tests
Doctors love handson tasks. Theyll ask you to:
- Perform a fingertonose test while looking at a targetmisses hint at optic ataxia.
- Copy a simple clock or a complex sceneerrors reveal simultanagnosia.
- Shift gaze rapidly between two pointsdifficulty points to ocular apraxia.
Imaging & NeuroPhysiology
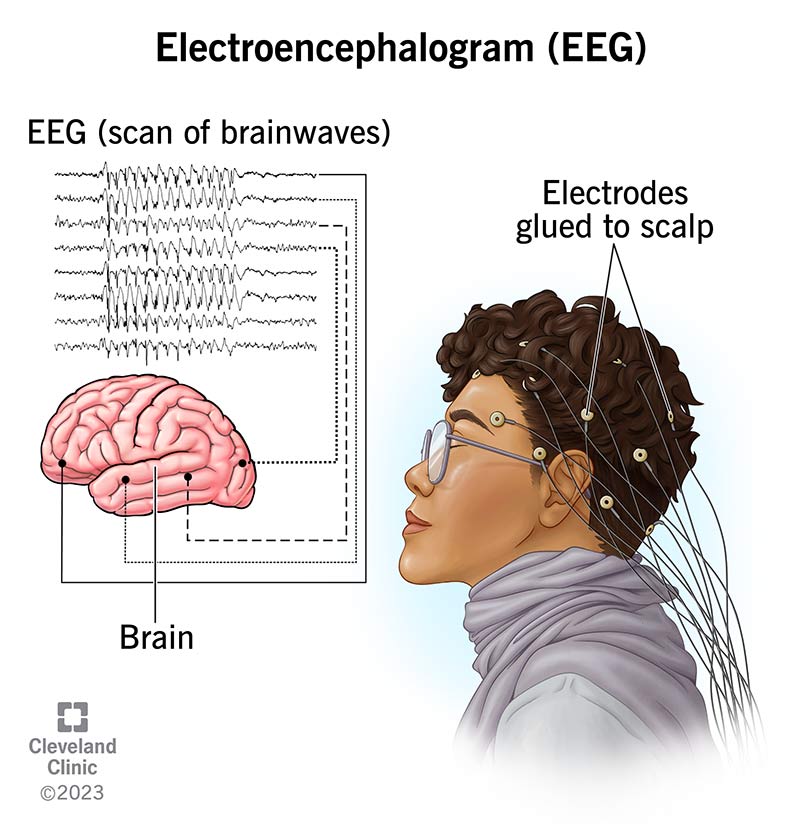
Imaging is the detectives magnifying glass. MRI (T2/FLAIR) usually shows the bilateral posterior lesions. In emergencies, a CT scan can catch acute bleed or edema. For researchlevel insight, functional MRI or PET scans map the metabolic slowdown in the affected cortex ().
Reading a Balinttype MRI Report StepbyStep
- Locate the posterior parietal lobes on axial slices.
- Look for symmetric hyperintensity or atrophy.
- Verify involvement of the occipital cortex.
- Correlate imaging with the clinical triad.
Treatment Options
Acute Care (PostStroke or Trauma)
If the damage is freshthink stroke or a recent head injuryspeed matters. Doctors may prescribe antiplatelet agents, steroids for swelling, or clotbusting meds, depending on the cause. But the real gamechanger is neurorehabilitation. Occupational therapists work on visualspatial drills, while physiotherapists guide safe reaching exercises.
LongTerm Strategies
Recovery isnt always a quick sprint; its more like a marathon with helpful pitstops:
- Compensatory techniques: Scanandstop eyemovement drills train you to pause, look, then movetackling ocular apraxia headon.
- Assistive technology: Audiotactile devices give auditory cues when youre reaching, and virtualreality games can make visualspatial practice fun.
Sample HomeExercise Routine (4Week Plan)
| Week | Exercise | Goal |
|---|---|---|
| 1 | Penciltracking on a grid (5min) | Improve oculomotor control |
| 2 | Reachforobjects in varying lighting | Reduce optic ataxia |
| 3 | Dualobject findthepair game | Train simultanagnosia |
| 4 | Realworld navigation (grocery aisle) | Transfer gains to daily life |
According to a guideline from the Cleveland Clinic, consistent, taskspecific training can boost functional outcomes even when the underlying brain damage is permanent. The key is patience and repetition.
Bottom Line
Understanding that Balints syndrome is tied to bilateral posterior brain damage gives you a solid footing for both diagnosis and rehab. The upside? Knowing the exact brain regions lets clinicians target therapy, and patients gain a roadmap for what to expect. The downside? Some causeslike neurodegenerative diseasesoffer limited reversal, so early detection is vital.
Bottom line: if you or someone you love shows the hallmark symptomsmissed reaches, stuck gaze, or trouble seeing multiple items at oncedont wait. A quick check with a neurologist or neuroophthalmologist can set the wheels in motion for the right treatment plan. If insurance coverage or treatment access is a concern, resources that explain Exondys 51 insurance navigation may be a model for how to approach coverage conversations with insurers.
Conclusion
Weve covered a lot: the brain areas behind Balints syndrome, why the triad disrupts ordinary life, how doctors pinpoint the damage, and what you can do daytoday to reclaim independence. Remember, the brain is resilient, and targeted rehabilitation can make a real difference, especially when the root cause is acute (stroke, trauma). If youre navigating this territory, keep the conversation open with your healthcare team, stay curious, and dont hesitate to ask questionsyour brains backstage crew deserves a supportive audience.
FAQs
What brain area is most commonly damaged in Balint's syndrome?
Balint's syndrome is most commonly associated with bilateral damage to the parietooccipital cortex, particularly involving regions around the parietal and occipital lobes.
What are the core symptoms of Balint's syndrome?
The classic triad includes optic ataxia (difficulty reaching for objects), ocular apraxia (difficulty shifting gaze), and simultanagnosia (inability to perceive multiple objects simultaneously).
What are common causes of the brain damage leading to Balint's syndrome?
Common causes include bilateral ischemic strokes affecting the posterior parietal and occipital lobes, traumatic brain injury, and certain neurodegenerative diseases such as Lewy body dementia.
How is Balint's syndrome diagnosed clinically?
Diagnosis involves bedside tests assessing visual-motor coordination and eye movements, like finger-to-nose testing for optic ataxia, gaze shifting tasks for ocular apraxia, and copying complex scenes to detect simultanagnosia, along with brain imaging such as MRI.
What treatment approaches help patients with Balint's syndrome?
Treatment focuses on neurorehabilitation with visual-spatial training, occupational therapy, and assistive technologies, as well as addressing the underlying cause like stroke or trauma to optimize recovery.