Arthrogryposis isnt one mysterious curse that just appears out of nowhere. In most cases it starts with reduced movement in the womb doctors call this fetal akinesia. That lack of motion, combined with a handful of genetic, neurological, or environmental factors, leads to the stiff joints we see after birth. Knowing the why helps families and clinicians plan the right care, manage expectations, and, most importantly, keep hope alive.
Fetal Akinesia Explained
What is fetal akinesia and how does it affect joint development?
Think of a baby in the uterus as a tiny gymnast. The constant kicking, stretching, and flexing are essential for shaping muscles, tendons, and joint capsules. When those movements are limited, the soft tissues dont get the exercise they need, and they end up tighteninghence the contractures that define arthrogryposis.
Primary medical sources that link akinesia to arthrogryposis
Leading pediatric centers such as and consistently cite fetal akinesia as the core mechanism. Their research shows that when fetal movement falls below a critical threshold, the risk of joint contractures rises sharply.
Realworld anecdote
When Mayas son was 20 weeks gestation, her obstetrician noticed unusually still ultrasound images. A followup scan confirmed markedly reduced limb motion. After birth, Maya learned that her babys stillness was the first clue to arthrogryposis. Mayas story reminds us that early detection, even if unsettling, can open the door to early therapy.
Genetic Factors Overview
Known gene mutations
About 2030% of arthrogryposis cases are linked to specific gene changes. The most common culprits include MYH3, PIEZO2, and TPM2. These genes influence muscle development, nerve signaling, or the elasticity of connective tissue.
How genetics interact with fetal movement
When a mutation disrupts the nerves that tell muscles to move, the babys limbs may stay relatively still, feeding back into the fetal akinesia cycle. In other words, the genetics dont act alonethey amplify the movement problem.
| Gene | Inheritance Pattern | Typical Impact on Movement |
|---|---|---|
| MYH3 | Autosomal dominant | Severe contractures of the elbows and knees |
| PIEZO2 | Autosomal recessive | Reduced sensation leading to limited fetal kicking |
| TPM2 | Autosomal dominant | Distal joint stiffness (hands & feet) |
Expert insight
Dr. Elena Ramirez, a pediatric geneticist at Seattle Childrens Hospital, explains that identifying a genetic mutation early lets us tailor physiotherapy and, in the future, consider genetargeted therapies. Her words underline why a genetic workup is often part of the diagnostic pathway.
FAQs Is arthrogryposis genetic?
In short, yes, it can be, but not always. When a hereditary mutation is found, families benefit from genetic counseling to understand recurrence risks. When no mutation surfaces, the condition is usually categorized as nongenetic fetal akinesia.
Maternal & Environmental Risks
Low amniotic fluid (oligohydramnios)
Amniotic fluid cushions and allows the baby to move freely. When fluid levels drop, the womb becomes cramped, and the fetus cant stretch out its limbs. This physical restriction can independently trigger arthrogryposis, even without a genetic cause.
Maternal infections, medications, or metabolic disorders
Severe maternal illnessessuch as uncontrolled diabetes, certain viral infections, or highdose corticosteroid treatmentscan interfere with fetal neuromuscular development. A concise list from Johns Hopkins Medicine includes:
- Maternal hypertension
- Rheumatic fever or other systemic infections
- Use of teratogenic drugs (e.g., some antiepileptics)
- Severe maternal malnutrition
Case study
Laura, who faced chronic hypertension throughout pregnancy, learned after her daughters birth that the reduced blood flow contributed to oligohydramnios and, consequently, arthrogryposis. While the diagnosis was bittersweet, early physical therapy helped Lauras daughter achieve functional milestones that many thought impossible.
Types of Arthrogryposis
Arthrogryposis multiplex congenita (AMC)
AMC is the umbrella term most clinicians use. It means multiple joint contractures present at birth. It doesnt point to a single cause; instead, it groups together all the different pathsgenetic, neurologic, or environmentalthat lead to the same outward signs.
Other listed subtypes
Beyond AMC, doctors distinguish several subtypes based on which muscles are affected and how severe the contractures are. The most common ones include:
| Type | Typical Cause(s) | Key Symptoms | Prognosis |
|---|---|---|---|
| Distal Arthrogryposis | Genetic (e.g., MYH3) | Stiffness in hands and feet | Generally good with therapy |
| Amyoplasia | Fetal akinesia, often unknown | Upper limb contractures, weak muscles | Variable; early intervention crucial |
| Complex Camptodactyly | Connectivetissue genes | Curved fingers, often bilateral | Manageable with splinting |
Why type matters for treatment planning
Knowing whether a child has distal arthrogryposis versus amyoplasia can change the therapeutic focusfrom intensive hand therapy to broader orthopedic surgery. Thats why clinicians push for a precise diagnosis early on.
Treatment by Cause
Physical & occupational therapy the universal first line
Even when the root cause is genetic, regular stretching, splinting, and activitybased programs can keep joints supple and improve functional reach. Think of therapy as a daily maintenance routine that prevents the contractures from becoming permanent.
Surgical interventions when structural issues demand it
In severe caseslike a fixed elbow contracture that blocks feedingsurgeons may perform tendon releases or joint realignments. A simple flowchart helps illustrate the decision process:
- Diagnose underlying cause
- Assess range of motion
- Begin with therapy; if no improvement
- Consider surgery
- Postop rehab to lock in gains
Emerging therapies linked to specific genetic causes
Researchers are exploring geneediting techniques for mutations like PIEZO2. While still experimental, early animal models suggest that correcting the genetic bug could restore normal nerve signaling and, eventually, fetal movementa true gamechanger for future families. For readers interested in related concepts of remission and long-term disease control in chronic musculoskeletal conditions, resources on ankylosing spondylitis remission may offer useful parallels in monitoring, criteria, and treatment goals.
Quick answer for readers searching arthrogryposis treatment
Most children benefit from a combination of early physical therapy, customized orthotic devices, and, when needed, surgical release. The exact mix depends on the cause and the severity of the contractures.
Life Expectancy Outlook
General life expectancy overview
For the overwhelming majority of individuals with arthrogryposis, life expectancy is normal. The condition itself rarely shortens lifespan; its the associated complications (like respiratory issues) that can affect outcomes.
How the underlying cause influences longterm outlook
If a childs arthrogryposis stems from an isolated genetic mutation with no systemic involvement, their prognosis is excellent. Conversely, when the contractures are part of a broader syndrome that includes heart or lung problems, careful monitoring becomes essential.
Realworld example
Jenna, now 22, was born with distal arthrogryposis affecting her hands and feet. With early therapy and a few minor surgeries, she graduated college, works as a graphic designer, and lives an independent life. Her story illustrates that disability often depends on the support network and the right interventions.
FAQstyle snippet
Is arthrogryposis a disability? It can be, especially if contractures limit mobility or daily tasks, but many individuals lead active, independent lives. Early, personalized care makes a huge difference.
Further Reading Links
For those who want to dive deeper, the following reputable sources offer comprehensive overviews, uptodate research, and patientfocused resources:
Remember, knowledge is power. Understanding the why behind arthrogryposis equips families with the tools to advocate for the right care, plan for the future, and keep hope alive.
Conclusion
In a nutshell, arthrogryposis usually begins with fetal akinesia, but the story doesnt end there. Genetic mutations, maternal health, and environmental factors can each add a layer to the condition, shaping everything from the type of contractures you see to the treatment path you follow. By grasping these causes, families can work handinhand with clinicians to choose therapies that fit their childs unique situation, keep expectations realistic, and celebrate every milestonebig or small. If youve walked this road or are just starting to learn, wed love to hear your thoughts. Share your experiences, ask questions, or simply let us know what helped you most. Youre not alone, and together we can turn complexity into confidence.
FAQs
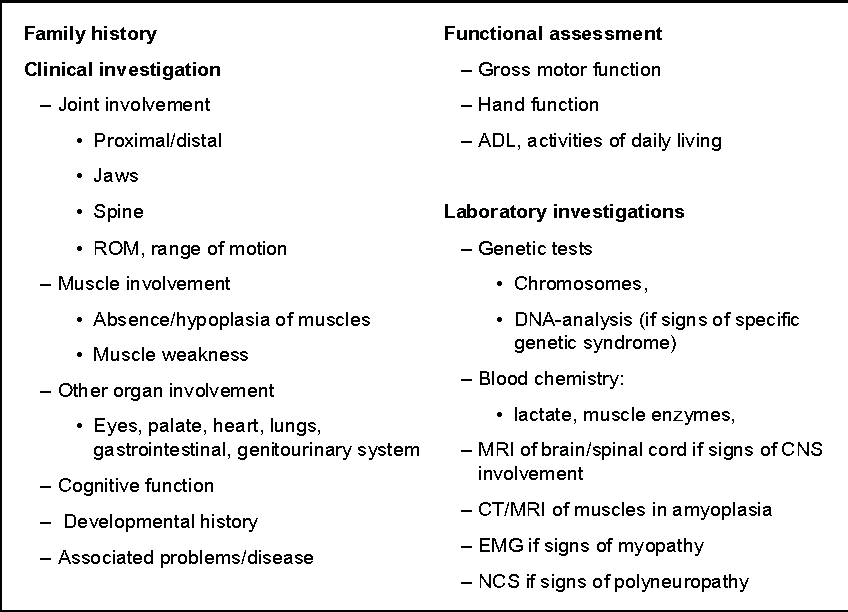
What is fetal akinesia and why does it lead to arthrogryposis?
Fetal akinesia is reduced movement of the baby in the womb. Without normal kicking and stretching, muscles, tendons, and joint capsules don’t develop properly, resulting in stiff, contracted joints characteristic of arthrogryposis.
Which genes are most commonly linked to arthrogryposis?
The genes MYH3, PIEZO2, and TPM2 account for about 20‑30 % of cases. Mutations affect muscle formation, nerve signaling, or connective‑tissue elasticity, often amplifying the fetal movement problem.
Can maternal health issues cause arthrogryposis?
Yes. Conditions such as oligohydramnios (low amniotic fluid), uncontrolled diabetes, hypertension, infections, or exposure to certain medications can restrict fetal movement and contribute to joint contractures.
What treatment options are available for a child diagnosed with arthrogryposis?
Early physical and occupational therapy is the first line of care. Depending on severity, orthotic devices, tendon releases, joint realignments, or emerging gene‑targeted therapies may be added.
Does arthrogryposis affect life expectancy?
For most individuals, life expectancy is normal. The condition itself rarely shortens lifespan; complications such as respiratory or cardiac involvement in broader syndromes may require additional monitoring.