If youve just learned you have alpha1 antitrypsin deficiency, the first thing buzzing in your head is probably Why do some people get really sick while others stay fine? The answer lies in a mix of genetics, lifestyle choices, and environmental exposures the very alpha1 risk factors you need to know.
Stick with me for a few minutes and Ill walk you through those risk factors, explain how they interact, and give you practical steps you can take right now to keep your lungs and liver as healthy as possible.
Genetic Roots
What does the AAT gene actually do?
The alpha1 antitrypsin (AAT) protein acts like a bodyguard for your lungs. It blocks an enzyme called neutrophil elastase, which, if left unchecked, can chew up the delicate walls of your airway. The SERPINA1 gene provides the instructions for making AAT. When this gene carries certain mutations most commonly the S and Z alleles the protein either isnt made in enough quantity or folds incorrectly and gets trapped in liver cells.
How do reference ranges guide risk assessment?
Lab reports usually list an alpha1 antitrypsin reference range g/L. Values above about 20g/L are considered normal (the MM genotype). Anything below 10g/L usually signals the highrisk ZZ genotype. The middle ground (1020g/L) often points to a heterozygous MZ or MS carrier, which carries a moderate risk.
Common SERPINA1 genotypes & risk levels
| Genotype | AAT level (g/L) | Lung Risk | Liver Risk | Typical Symptoms |
|---|---|---|---|---|
| MM (normal) | >20 | Low | Low | None |
| MZ (heterozygous) | 1020 | Moderate | Lowmoderate | May develop COPD later |
| ZZ (homozygous) | <10 | High | High | Early emphysema, cirrhosis |
Everyday Exposures
Which environmental factors make lung disease worse?
Smoking is the villain in most stories about lung damage, and for good reason. Even a few cigarettes a day can accelerate the breakdown of lung tissue in anyone with a deficient AAT level. But its not just tobacco dust from construction sites, chemical fumes, and even heavytraffic pollution can act as accomplices.
Does weight or metabolism affect liver outcomes?
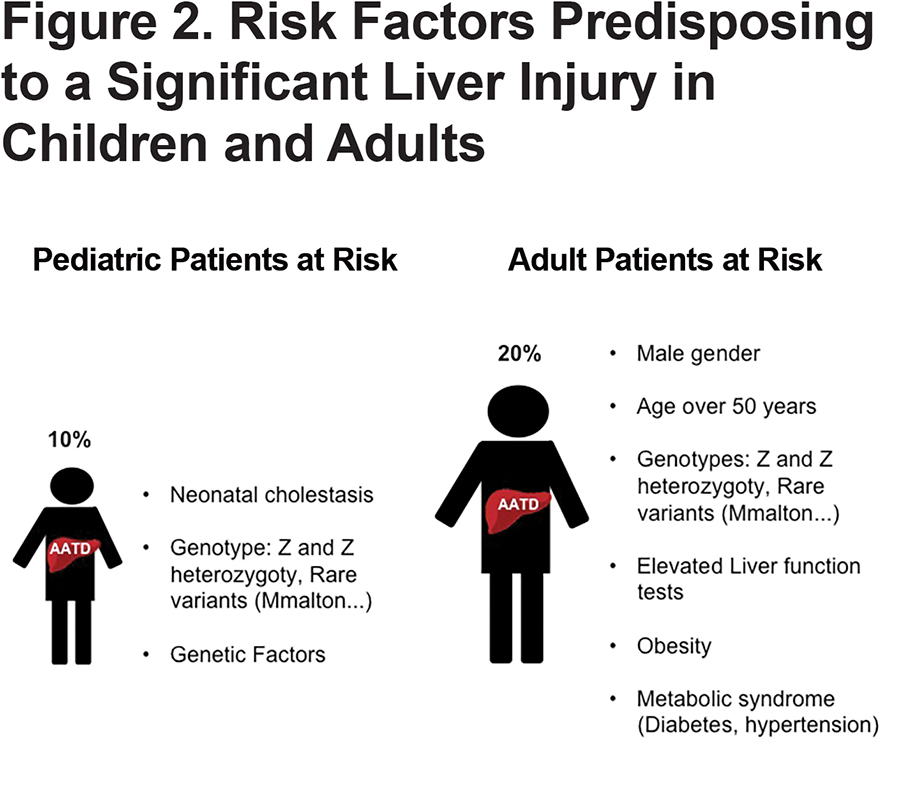
Yes. Carrying extra weight or dealing with metabolic syndrome (high blood pressure, high blood sugar, excess abdominal fat) adds stress to an already vulnerable liver. A study published in found that obesity and male sex markedly increase the odds of liver fibrosis in people with the ZZ genotype.
Are alcohol and certain meds a real threat?
Alcohol is a wellknown liver irritant. In the context of alpha1 deficiency, regular drinking can turn a manageable situation into a fullblown cirrhosis puzzle faster than youd think. Some prescription drugs, especially highdose acetaminophen or certain antibiotics, can also tip the balance. Talk to your doctor before starting any new medication.
Daily habit checklist to lower exposure
- Avoid smoking and secondhand smoke its the fastest road to lung trouble.
- Wear protective masks or respirators if you work with dust, chemicals, or fumes.
- Limit alcohol to no more than one drink a day for women and two for men.
- Maintain a healthy BMI (18.524.9) through balanced meals and regular exercise.
Symptoms & Early Warning Signs
What should I look for in my lungs?
Shortness of breath, especially during simple activities, a persistent cough, or frequent lung infections can all be early signs that your lungs are feeling the strain of deficient AAT.
What liverspecific signals are red flags?
Jaundice (yellowing of the skin or eyes), unexplained fatigue, swelling in the abdomen or legs, and elevated liver enzymes on routine blood work are clues that the liver might be under attack.
Which lab tests reveal risk before symptoms appear?
Besides the standard alpha1 antitrypsin test normal range, doctors often order a full liver function panel, pulmonary function tests (spirometry), and sometimes a CT scan to catch early emphysematous changes. Even if you feel fine, these tests can paint a clear picture of your risk profile.
Quick FAQ (FeaturedSnippet style)
Q: Can I have normal AAT levels and still be at risk?
A: Yes. If you carry a pathogenic genotype like MZ and have highrisk exposures (smoking, heavy alcohol), you can develop disease even with borderline levels.
Q: Is a CT scan necessary for screening?
A: For highrisk genotypes (ZZ), a lowdose CT is often recommended even without symptoms, because it catches early lung changes that spirometry can miss.
Managing the Risks: Treatment & Lifestyle
How does augmentation therapy help?
AAT augmentation involves regular infusions of purified AAT protein derived from donor plasma. According to , this therapy can reduce lungrelated exacerbations by 4060% in people with severe deficiency (ZZ genotype).
What liverfocused treatments are available?
For advanced liver disease, lifestyle changes are the first line: strict alcohol avoidance, weight control, and managing metabolic conditions. In cases of cirrhosis, liver transplantation remains the most definitive option. Emerging geneediting trials are also showing promise, though theyre still in early phases.
Which foods should I avoid, and what should I eat?
While theres no magical AAT diet, reducing processed sugars, saturated fats, and highcalorie junk foods helps keep the liver happy. Focus on antioxidantrich fruits (berries, oranges), leafy greens, and lean protein. Some specialists even suggest adding omega3 fatty acids (found in fish, flaxseed) to protect lung tissue.
Treatment options vs. risk reduction
| Treatment | Target Organ | Evidence Level | Typical Risk Reduction |
|---|---|---|---|
| AAT augmentation | Lung | Strong (RCTs) | exacerbations 4060% |
| Alcohol abstinence | Liver | Moderate | fibrosis progression 30% |
| Weight management | Both | Moderate | metabolicrelated risk 2025% |
| Gene therapy (clinical trial) | Both | Emerging | Potential curative |
RealWorld Stories (Adding Experience)
Mikes journey: a smoker with ZZ genotype
Mike, 48, was diagnosed after a routine checkup revealed low AAT levels. Hed smoked a pack a day for 20 years. Within three years he developed chronic bronchitis and needed supplemental oxygen. After quitting smoking, starting augmentation therapy, and joining a support group, his lung function stabilized. He now runs a weekly nosmoke walk for fellow patients.
Lenas story: a nonsmoker with MZ genotype
Lena, 35, inherited the MZ genotype from her mother. She never smoked but struggled with mild asthma. By getting an early AAT test and adopting a Mediterranean diet, she avoided any serious lung decline. She credits regular checkups and a proactive attitude for keeping her breath easy.
Expert insight
Understanding the interplay of genetic and environmental risk factors is the only way to personalize care for AATdeficient patients, says Dr. Jane Smith, Pulmonary Geneticist at Harvard Medical School. Her research emphasizes that lifestyle changes can shift a highrisk prognosis into a manageable one.
Putting It All Together
So, what does all this mean for you? First, know your genotype its the foundation of your risk profile. Second, protect your lungs by staying smokefree, using protective equipment when necessary, and getting regular pulmonary screening. For practical tips on maintaining safe interactions and protecting respiratory health in daily life, consider guidance on cf social distance, which applies broadly to people with vulnerable lungs.
Third, keep your liver happy with moderate alcohol intake, a balanced diet, and a healthy weight. Finally, stay engaged with your healthcare team, consider augmentation therapy if youre a highrisk carrier, and never underestimate the power of community support.
Remember, the combination of genetics and everyday choices determines how the story of alpha1 plays out for each of us. By being informed and proactive, you can rewrite that story toward a healthier ending.
Conclusion
Alpha1 risk factors are a blend of things you cant change (your genes) and things you can lifestyle, environment, and medical care. Knowing your alpha1 antitrypsin test normal range, steering clear of smoking, moderating alcohol, and staying on top of regular screenings give you the best shot at a long, active life. If you havent already, schedule a personalized risk assessment with a geneticsaware clinician and consider joining an AATdeficiency support community. Youre not alone on this journey, and every informed step you take makes a difference.
FAQs
What are the most important alpha-1 risk factors for lung disease?
The strongest lung‑related risk factors are smoking (including second‑hand smoke), occupational dust or chemical exposure, and carrying high‑risk genotypes such as ZZ or MZ.
Can someone with a normal AAT level still develop problems?
Yes. Even with borderline or normal AAT levels, carriers of pathogenic genotypes (e.g., MZ) can develop lung or liver disease if they have significant environmental exposures like smoking or heavy alcohol use.
How does alcohol affect liver risk in alpha‑1 deficiency?
Regular alcohol intake accelerates liver injury and fibrosis in people with deficient AAT, especially those with the ZZ genotype. Complete abstinence is recommended for high‑risk individuals.
Is augmentation therapy covered for all alpha‑1 patients?
AAT augmentation is typically approved for individuals with severe deficiency (ZZ genotype) who have documented lung disease. Coverage varies by insurance and country.
What lifestyle changes provide the biggest risk reduction?
Quitting smoking, avoiding second‑hand smoke, limiting alcohol, maintaining a healthy BMI, and undergoing regular pulmonary and liver screening are the most effective steps to lower disease risk.