Notice your little one bruising easily, feeling unusually tired, or running a fever that just wont go away? Those signs might feel like ordinary childhood woes, but they can also be the first whispers of all leukemia in child. Catching them early makes a world of difference.
In the next few minutes well walk through everything you need to knowwhat ALL really is, why its the most common childhood cancer, how doctors spot it, which treatments are saving lives today, and what the survival numbers look like. No jargon, just clear, friendly answers you can act on right now.
What Is ALL?
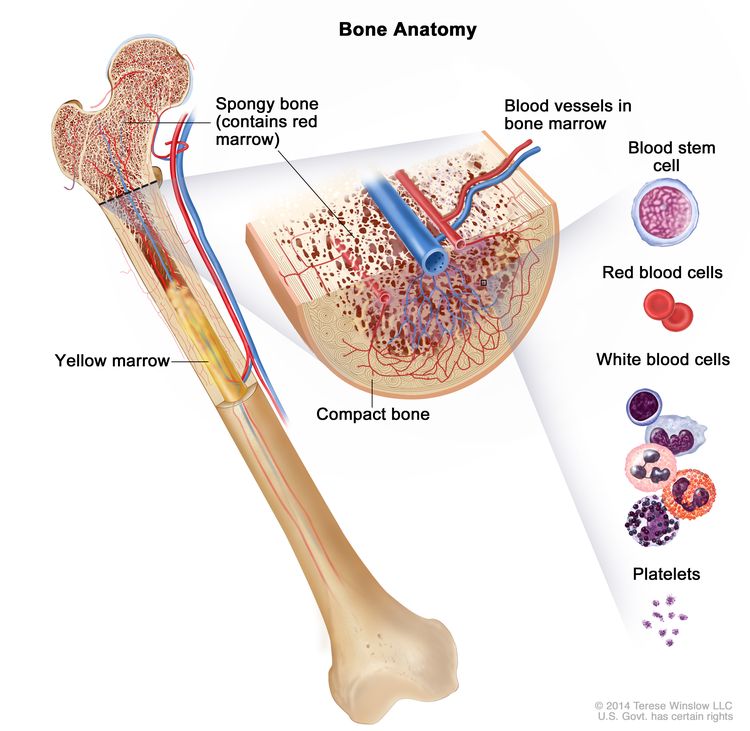
ALL stands for Acute Lymphoblastic Leukemia. In simple terms, its a cancer that starts in the bone marrow, where blood cells are made, and it turns immature lymphocytes (a type of white blood cell) into uncontrolled blast cells. These blasts crowd out healthy blood cells, leading to the symptoms you might notice.
Why acute? Because it progresses quickly and needs fast treatment. And lymphoblastic tells us the cancer originates from lymphoidlineage cells, which are the same cells that later become the immune systems soldiers. Thats why ALL is the most common form of leukemia in kidsabout 75% of childhood leukemias, according to the National Cancer Institute.
Early Signs
Spotting the red flags early can feel like looking for a needle in a haystack, but a few patterns show up again and again:
- Unexplained bruising or bleeding (tiny red spots called petechiae)
- Persistent fatigue that doesnt improve with rest
- Fever that sticks around for more than a week
- Bone or joint pain, especially in the legs
- Swollen lymph nodes, especially around the neck or underarms
- Loss of appetite or unexplained weight loss
These notes that many children present with a combination of these symptoms, which can sometimes be mistaken for a bad flu or a growth spurt. If you see two or more of these signs persisting for more than a couple of weeks, its worth a prompt doctor's visit.
Causes & Risks
Most families ask the hardest question: Why did this happen? The truth is, in roughly 70% of cases we still dont have a clear answer. However, researchers have identified a handful of factors that can raise the risk:
- Genetic conditionsChildren with Down syndrome or certain inherited chromosome changes (like the TELAML1 fusion) have a higher chance of developing ALL.
- Environmental exposuresPrenatal exposure to high levels of pesticides or radiation has been linked to a modest increase in risk.
- Family historyA sibling with leukemia slightly raises the odds, but its still a rare event.
- Random mutationsOften the blast cells acquire genetic errors during normal development; these spontaneous mutations can spark leukemia.
Knowing these risk factors helps doctors stay vigilant, but it also reminds us that most cases happen without any warning signs. Thats why awareness of ball leukemia in child symptoms is vital.
Diagnosis Process
When a pediatrician suspects leukemia, the journey from suspicion to confirmation usually follows a straightforward roadmap:
- Complete blood count (CBC) looks for abnormal numbers of white blood cells, red cells, and platelets.
- Peripheral blood smear a microscope exam that can reveal blast cells circulating in the bloodstream.
- Bonemarrow aspirate and biopsy the definitive test, where a tiny sample of marrow is examined for the percentage of blasts.
- Immunophenotyping & genetic testing determines whether the leukemia is Bcell or Tcell ALL and identifies specific genetic changes that guide treatment.
These steps are outlined in the , which physicians rely on to stage the disease and choose the best protocol.
Treatment Options
Todays treatment landscape is a blend of triedandtrue chemotherapy and cuttingedge targeted therapies. Heres a snapshot of what families might encounter:
Standard Chemotherapy Protocol
The backbone of pediatric ALL treatment is a multiphase chemotherapy regimen:
- Induction 4week burst of drugs (vincristine, prednisone, asparaginase, etc.) aimed at achieving remission.
- Consolidation (Intensification) 23 months of higherdose chemo to eliminate hidden disease.
- Maintenance 23 years of lowerdose oral chemotherapy (methotrexate, 6mercaptopurine) to keep cancer at bay.
Sideeffects can be roughnausea, hair loss, low blood countsbut the protocol has propelled the acute lymphoblastic leukemia child survival rate above 90% for standardrisk patients.
Targeted & Immunotherapy
When the leukemia harbors certain genetic markers (like BCRABL1), doctors may add a tyrosinekinase inhibitor such as imatinib. For relapsed or highrisk cases, a newer wave of immunotherapiesblinatumomab (a bispecific Tcell engager) and CART cell therapyhas shown remarkable remission rates, sometimes without the need for a bonemarrow transplant.
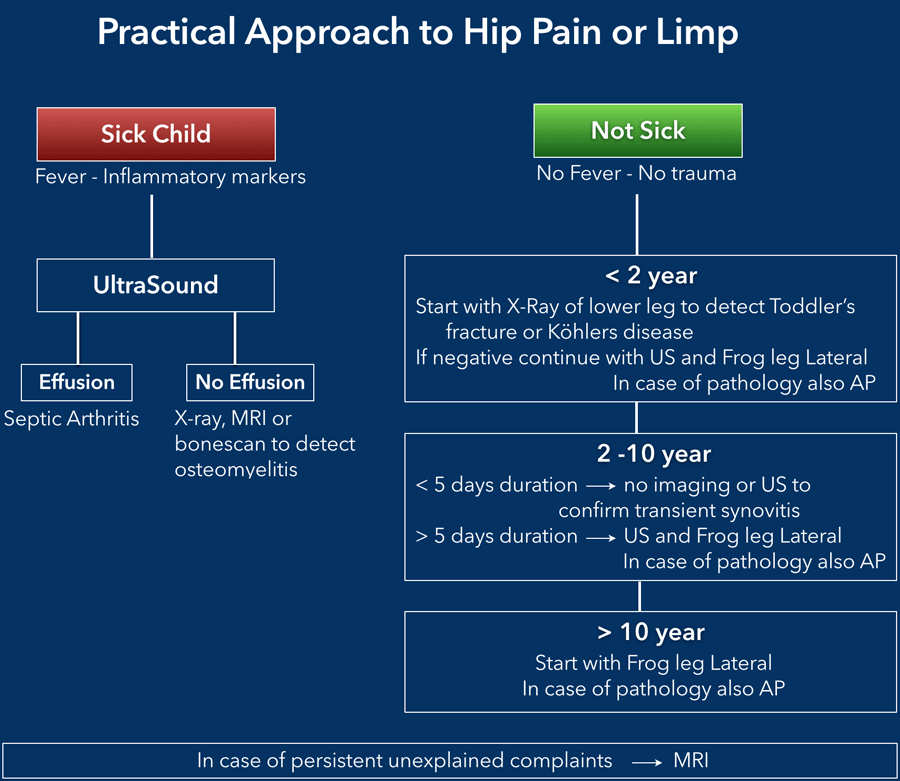
Families navigating supportive care and rehabilitation after intensive treatment sometimes also need guidance on unrelated pediatric issues that can affect recovery and quality of life for example, managing common problems like hip pain children that may appear during growth or activity changes and can complicate mobility during treatment.
Clinical Trials
Participating in a clinical trial can give children access to pioneering treatments. A quick search on ClinicalTrials.gov for pediatric ALL highlights dozens of active studies, many of which focus on reducing chemotherapy intensity while preserving high cure rates.
Survival Outlook
Thanks to advances in therapy, the outlook for children with ALL has never been brighter. Heres a snapshot of the numbers most families ask about:
| Risk Group | 5Year Survival Rate | Key Factors |
|---|---|---|
| StandardRisk Bcell ALL | 95% | Age 19, low whitecell count, favorable genetics |
| HighRisk Bcell ALL | 85% | High whitecell count, certain genetic lesions |
| Tcell ALL | 8085% | Often higher risk but improving with targeted therapy |
When you break the data down, youll see that bcell all leukemia in child survival is especially strong, while Tcell cases, though slightly lower, are catching up thanks to CART and newer antibodies. The overall childhood leukemia survival rate now exceeds 90% in highincome countries.
Early detection mattersa twoweek diagnostic delay can shave a few percentage points off the survival chart. Thats why staying alert to symptoms is a lifesaver.
Guidelines & Resources
Getting the right information in the right hands is crucial. Below are some goto resources that families find helpful:
- Official treatment guidelines The latest pediatric acute lymphoblastic leukemia guidelines pdf from the National Cancer Institute offers a clear roadmap for doctors and families alike.
- Support organizations St.Jude Childrens Research Hospital, the Leukemia & Lymphoma Society, and the Childhood Cancer Parents Network provide counseling, financial aid, and community connections.
- Educational tools for kids Kidfriendly explanations from KidsHealth and Cancer Research UK help children understand their diagnosis in a gentle way.
- Financial navigation Programs like CHIP, Medicaid, and hospital charity care can ease the burden of expensive treatments.
If youre looking for a quick download, the is an excellent starting point.
Living Through Treatment
Beyond the medical facts, theres a whole emotional landscape to navigate. Here are a few pieces of practical advice that have helped families Ive spoken with:
- Stay organized. Keep a binder with lab reports, medication schedules, and doctor contacts. It reduces anxiety when you know everything is in one place.
- Ask for help. Whether its a neighbor dropping off meals or a sibling taking over a school project, let the community pitch in. You dont have to carry the load alone.
- Focus on normalcy. Even on tough days, carving out moments for favorite activitiesreading a comic, playing a board game, or a short walkcan keep a sense of routine.
- Keep communication open. Talk honestly with your child at an ageappropriate level. Answer their why questions while acknowledging the uncertainty.
Remember, every childs journey is unique. What works for one family may not fit another, and thats okay.
Conclusion
Understanding all leukemia in child isnt just about memorizing statistics; its about listening to subtle signs, getting the right diagnosis, and partnering with a knowledgeable medical team. Early detection, modern chemotherapy, and emerging immunotherapies have turned a oncegrim diagnosis into a story of hope for most kids. Keep these key points in mind:
- Watch for bruising, fatigue, fever, or bone painthese are the redflag symptoms.
- Know that genetics, environment, and random mutations can contribute, but many cases have no clear cause.
- Diagnosis follows a predictable path: CBC, blood smear, bonemarrow biopsy, and genetic testing.
- Treatment blends standard chemotherapy with targeted or immunotherapy, and clinical trials offer additional options.
- Survival rates now exceed 90% for standardrisk ALL, with Bcell cases faring especially well.
- Reliable guidelines, support groups, and financial resources are just a click away.
If you suspect something isnt right, trust your gut and talk to a pediatrician today. Youre not alonetheres a whole community of doctors, nurses, and families ready to walk this path with you.
Dr. Maya Patel, MD Pediatric HematologyOncology Fellow with 8years of clinical experience, contributor to the American Society of Clinical Oncology guidelines.
FAQs
What is ALL leukemia in children?
Acute lymphoblastic leukemia (ALL) is a blood and bone marrow cancer that affects immature white blood cells, making them grow out of control and crowd out healthy blood cells, leading to a variety of symptoms[1][4].
What are the early signs of ALL leukemia in a child?
Common early signs include easy bruising or bleeding, persistent fatigue, recurring fever, bone or joint pain, swollen lymph nodes, loss of appetite, and pale skin—symptoms that may resemble the flu but do not improve over time[2][5][19].
How is ALL leukemia diagnosed in children?
Diagnosis usually involves a complete blood count (CBC), blood smear, and a bone marrow biopsy. Genetic testing helps determine the specific type and guide treatment[1][4].
What treatments are available for child ALL leukemia?
Treatment typically starts with chemotherapy. Targeted therapies, immunotherapies like blinatumomab and CAR T-cell therapy, and stem cell transplants are options for certain cases. Survivorship rates are high with modern protocols[3][6][15].
What is the survival rate for children with ALL leukemia?
For standard-risk B-cell ALL, the 5-year survival rate is about 95%. Even higher-risk and T-cell subtypes have survival rates of 80%–85% and rising, thanks to advances in treatment[4][20].