Quick Answers
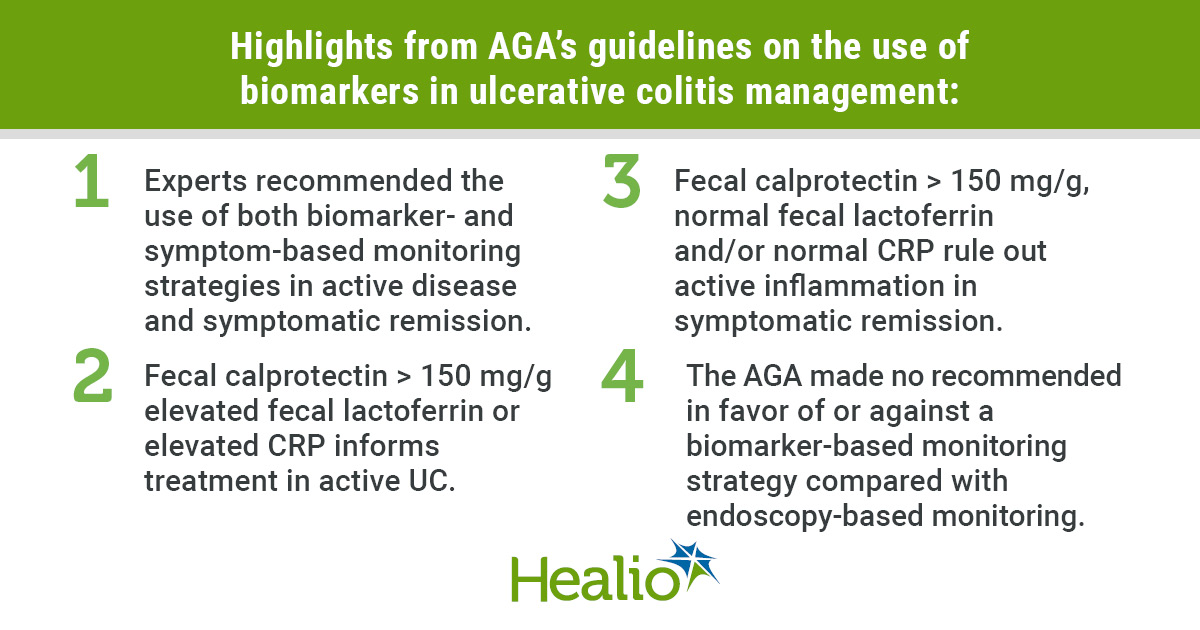
What does the AGA say?The 2022 AGA clinical practice guideline on the role of biomarkers for the management of ulcerative colitis recommends using fecal calprotectin, fecal lactoferrin, and serum Creactive protein (CRP) as the primary noninvasive tools to monitor disease activity, decide when to stepup therapy, and catch a flare before symptoms get out of hand. For the full guideline summary see the AGA ulcerative colitis management guideline.
How often should I test?For patients who feel okay but have ulcerative colitis, the guideline advises a combined checkin of symptoms+biomarker testing every36months. If the biomarker level climbs, an endoscopic reassessment is recommended even if youre still feeling fine.
Why Biomarkers
Imagine trying to hear a whisper in a noisy roomthats what were doing when we rely only on symptoms. Biomarkers are the quiet whispers from your gut that tell you whether inflammation is bubbling beneath the surface.
What are noninvasive biomarkers?
Theyre labbased measurements you can obtain without an endoscope. The three the AGA highlights are:
- Fecal calprotectin a protein released by neutrophils that spikes when the colon is inflamed.
- Fecal lactoferrin another neutrophilderived protein, useful when calprotectin isnt available.
- Serum CRP a bloodbased marker that rises with systemic inflammation, especially in moderatetosevere disease.
How do they compare to colonoscopy?
Colonoscopy gives you a direct view, but its invasive, costly, and not something you want every few months. Studies show fecal calprotectin has a sensitivity of about85% and specificity near80% for detecting endoscopic inflammation. In other words, its a reliable early warning system that can spare you an unnecessary scope.
What does the AGA say?
The guideline, drafted by the , grades fecal calprotectin as a strong recommendation for routine monitoring. Lactoferrin gets a moderate endorsement, while CRP is suggested for severe cases or when stool samples are hard to obtain.
When should each marker be used?
- Acute flare Order fecal calprotectin plus CRP to gauge severity.
- Maintenance Check calprotectin (and optionally lactoferrin) every 36months.
- Pediatric patients Calprotectin works well; CRP is less reliable in children.
- Extensive disease (pancolitis) Both stool markers and CRP provide a fuller picture.
What are the limitations?
No test is perfect. A recent review warned that NSAIDs, infections, or even a recent bowel prep can falsely elevate calprotectin. Likewise, CRP may stay low in mild UC despite active inflammation. Thats why the AGA stresses trend monitoring rather than a single cutoff.
Practical Use
Lets move from theory to the daytoday. Below is a realworld workflow that you can copypaste into your clinics checklist.
How to order and interpret fecal calprotectin
1. Sample collection Give the patient a prefilled container, ask them to avoid bloodstreaked stools, and store the sample in the fridge if it wont reach the lab within 24hours.
2. Reference ranges Normal is <50g/g. Values 150250g/g suggest mild inflammation; >250g/g is usually a red flag for active disease.
3. Trend analysis A rise of 50100g/g from your baseline often precedes a clinical flare. If you see that, schedule a colonoscopy or consider stepping up therapy.
When to add fecal lactoferrin?
If the lab you use doesnt offer calprotectin, lactoferrin works almost as well. Use the same timing (every 36months) and interpret it with the same cutoffs: >200g/g flags active inflammation.
Serum CRP: role in severe disease
CRP rises quickly with systemic inflammation. A level >10mg/L in a UC patient often correlates with extensive colitis and may prompt earlier biologic escalation.
Algorithm: Biomarkerdriven monitoring schedule
| Step | What to do | When |
|---|---|---|
| 1. Symptom check | Ask about stool frequency, blood, urgency. | Every visit. |
| 2. Biomarker test | Order fecal calprotectin ( lactoferrin) + CRP if severe. | Baseline, then every 36months. |
| 3. Interpret | Stable <150g/g = continue current regimen. Increase 150250g/g = monitor closely. >250g/g = consider endoscopy and therapy escalation. | Immediately after results. |
| 4. Action | Discuss findings with patient, adjust meds, schedule scope if needed. | Within 1week of abnormal result. |
Integrating biomarkers with symptom scores
Combine the Mayo score (or Simple Clinical Colitis Activity Index) with the lab values. For example, a Mayo score of2plus calprotectin 180g/g may still warrant a colonoscopy, whereas a Mayo of4with a normal calprotectin might suggest functional symptoms rather than inflammation.
Guideline Comparison
Ever wonder whether the AGA is the only voice shouting about biomarkers? Lets line up the major societies sidebyside.
AGA vs. ACG
The American College of Gastroenterology (ACG) also endorses fecal calprotectin, but it places slightly less emphasis on routine testing in mild remission. Their 2021 statement calls the test useful when clinical uncertainty exists rather than a blanket recommendation.
AGA vs. ECCO
The European Crohn & Colitis Organisation (ECCO) aligns closely with the AGA on calprotectin thresholds but adds a note that lactoferrin is preferable in regions where calprotectin assays are not standardized.
What do the latest IBD guidelines say?
Across the board whether you read the AGA ibd guidelines, the latest ibd guidelines from the World Gastroenterology Organisation, or the crohn\'s flare management guidelines theres a consensus: noninvasive biomarkers are now the backbone of treattotarget strategies.
Consensus across societies
All three major bodies (AGA, ACG, ECCO) agree on three core points:
- Use fecal calprotectin as the firstline monitoring tool.
- Confirm rising biomarkers with endoscopy before major therapeutic changes.
- Interpret results in the context of symptoms and patient history.
Benefits & Risks
Nothing in medicine is allgood or allbad. Lets weigh the scales.
Benefits
- Early detection A rising calprotectin level often appears weeks before the patient feels worse.
- Reduced scopes By triaging based on biomarkers, you can spare patients unnecessary colonoscopies.
- Costeffectiveness Stool tests are cheap compared to an endoscopic suite.
- Patient empowerment Sharing numbers with patients makes the disease feel more tangible and controllable.
Risks / challenges
- False positives Infections, NSAIDs, or recent bowel prep can inflate results.
- Assay variability Different labs use different kits; always compare trends, not isolated numbers.
- Overtesting Testing every month can create anxiety without adding clinical value.
- Patient anxiety Some patients fixate on numbers. The guideline tells us to pair results with a calm conversation.
How the guideline mitigates risk
The AGA explicitly states: Biomarker testing should be coupled with symptom assessment; isolated elevations without clinical correlation should prompt repeat testing before invasive procedures. In plain English: dont jump to a colonoscopy the moment the lab spits out a high number.
Action Plan
Ready to turn knowledge into habit? Heres a stepbystep checklist you can copy into your EMR or notebook.
| Step | What to Do | Helpful Resource |
|---|---|---|
| 1. Baseline | Order fecal calprotectin, lactoferrin (if needed), and serum CRP at diagnosis. | |
| 2. Schedule | Set a reminder in the EMR for biomarker testing every 36months. | EMR workflow template. |
| 3. Interpret | Use the Biomarkerdriven monitoring schedule table to decide next steps. | Internal clinic algorithm. |
| 4. Communicate | Give patients a onepage What Your Test Means handout. | Patienteducation template. |
| 5. Escalate | If calprotectin >250g/g or CRP >10mg/L, arrange endoscopy and discuss therapy adjustment. | Biologic treatment pathways. |
And remember, the most powerful tool isnt the lab result its the conversation you have with your patient. A quick Hey, your numbers have nudged up a bit; lets talk about how youre feeling and what we can tweak goes a long way toward building trust.
Conclusion
The 2022 AGA clinical practice guideline makes it crystal clear: fecal calprotectin, lactoferrin, and serum CRP are now the cornerstones of ulcerative colitis monitoring. By weaving these noninvasive biomarkers into a routine symptom+test checkin, you can catch flares early, avoid unnecessary colonoscopies, and tailor therapy to each individuals disease rhythm. At the same time, staying aware of false positives and keeping the conversation patientcentered ensures you dont overreact to a single number. Grab the full guideline PDF, talk to your gastroenterology team about setting up a biomarker schedule, and take the first step toward smarter, kinder UC care today.
FAQs
What non‑invasive biomarkers does the AGA recommend for ulcerative colitis?
The guideline endorses fecal calprotectin, fecal lactoferrin, and serum C‑reactive protein (CRP) as first‑line tools for monitoring disease activity.
How often should a patient in remission have biomarker testing?
For stable patients, the AGA advises combined symptom assessment and biomarker testing every 3–6 months.
What calprotectin level indicates active inflammation?
Values > 250 µg/g usually signal active disease; 150–250 µg/g suggest mild inflammation, and < 50 µg/g is considered normal.
When should CRP be added to the monitoring panel?
CRP is most useful in moderate‑to‑severe ulcerative colitis or extensive (pancolitis) disease, especially when stool samples are unavailable.
What should be done if a biomarker rises but the patient feels fine?
The guideline recommends repeating the test to confirm a trend and, if it remains elevated, arranging endoscopic evaluation before changing therapy.