Quick Answer Summary
Did you know? Most adrenal cancers are caught at stageIIII using CT or MRI, but adding a PETCT can uncover hidden metastases in about15% of cases. Bottom line: a combined CT+MRIPET approach gives the clearest picture of the tumors size, local invasion, and distant spread, helping doctors choose the right treatment path.
In short, if you (or a loved one) are facing an adrenal mass, the radiology report isnt just a bunch of numbersits the roadmap that decides whether youre looking at a simple surgery or a more complex, multidisciplinary plan.
Overview of Staging
Why Staging Matters
Think of cancer staging like a weather forecast. Knowing whether a storm is just a drizzle or a fullblown hurricane changes how you prepare. With adrenal carcinoma, the stage tells you:
- Whether the tumor can be removed safely (surgery) or needs systemic therapy first.
- If you qualify for clinical trials that might offer cuttingedge treatments.
- What your 5year survival odds look likestageI is roughly80% survival, while stageIV drops to about15%.
Core Imaging Modalities
| Modality | Primary Role | Typical Findings | Key References |
|---|---|---|---|
| CT (contrastenhanced) | Firstline anatomic staging | Heterogeneous mass, >10cm, irregular borders, calcifications | |
| MRI | Softtissue characterization, vascular invasion | T1hypointense, T2hyperintense, loss of signal on outofphase | |
| PETCT (FFDG) | Detect distant metastasis, assess metabolic activity | Intense uptake in malignant lesions, helps differentiate from adenoma | |
| Ultrasound | Adjunct for biopsy guidance | Hypoechoic mass, limited staging utility | |
| Functional Imaging (CMTO, FFDOPA) | Rare, for refractory or hormonally active cases | Specifies hormoneproducing tumors |
StepbyStep Workflow
1 Initial Evaluation ContrastEnhanced CT
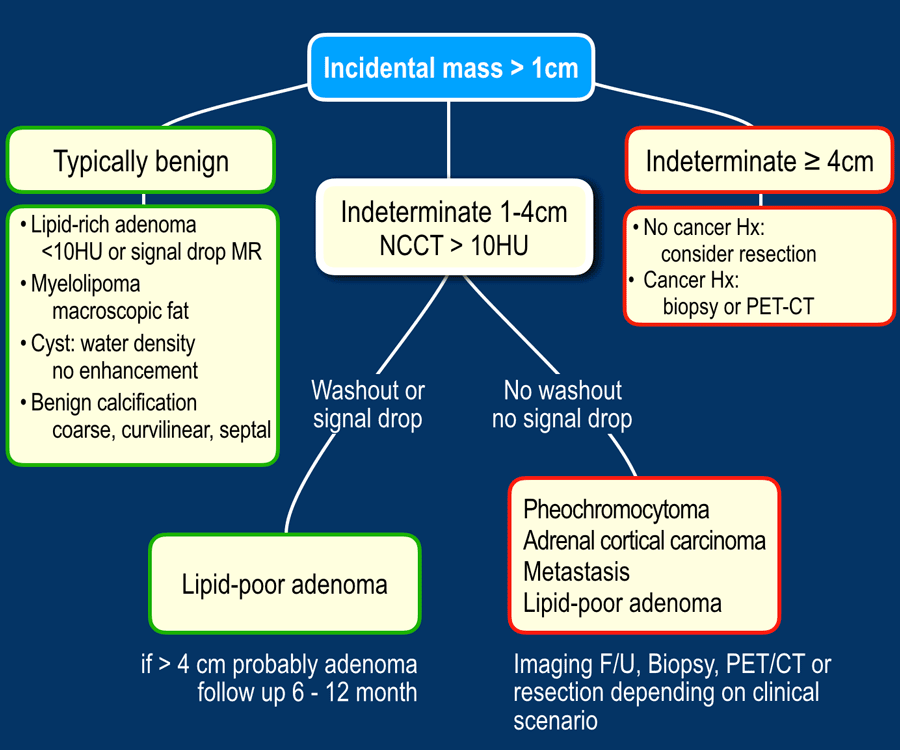
The journey usually starts with a multiphase CT scan (noncontrast, arterial, portalvenous). Radiologists will measure the mass, note its attenuation in Hounsfield Units (HU), and calculate the absolute washout. A washout >60% on delayed images usually points to a benign adenoma, while <60% raises suspicion for carcinoma. This is where the term adrenal washout radiology pops up.
2 ProblemSolving MRI (When CT Is Inconclusive)
If the CT cant tell whether the lesion is invading nearby vessels or if the washout numbers are borderline, we move to MRI. Key sequences include:
- Inphase/outofphase imaging to detect microscopic fat (helps separate adenoma from carcinoma).
- T2weighted lightbulb signbright on T2, often seen in pheochromocytoma (see pheochromocytoma vs adrenocortical carcinoma radiology).
- Diffusionweighted imaging (DWI)high signal suggests high cellularity, typical of malignancy.
3 WholeBody Staging PETCT or WholeBody MRI
For tumors larger than 5cm, high Ki67, or when you suspect spread beyond the adrenal gland, a PETCT is invaluable. It lights up distant siteslungs, liver, bonesgiving us the full picture of adrenal metastasis radiology. Some centers also use wholebody MRI for patients who cant receive radiation.
4 Ancillary Tests & Reporting Checklist
Beyond imaging, youll usually have a hormone panel (cortisol, aldosterone, catecholamines) to see if the tumor is functional. If the mass is nonresectable or appears atypical, a coreneedle biopsy under imaging guidance may be performedalways after a multidisciplinary discussion.
When you (or your doctor) write the final report, make sure it includes:
- Clinical question and indication.
- Technique (phases, sequences, contrast used).
- Findings size, attenuation, washout, invasion, nodal status, distant lesions.
- Impression stage according to radiologic criteria.
- Recommendations further imaging, referral to tumor board, possible biopsy.
Staging Systems Defined
| Stage | Radiologic Criteria (CT/MRI/PET) | Typical Prognosis |
|---|---|---|
| I | Tumor 5cm, confined to adrenal gland, no local invasion | 5year OS 80% |
| II | Any size with capsular invasion, no nodal spread | 5year OS 60% |
| III | Regional lymph node involvement or adjacent organ invasion (kidney, liver) | 5year OS 30% |
| IV | Distant metastasis (lung, bone, brain) on PETCT/CT | 5year OS 15% |
These criteria come from the American Cancer Societys staging guidelines and are the backbone of treatment planning.
Comparing Adrenal Lesions
Adrenal Adenoma vs. Carcinoma (Washout & ChemicalShift)
Adenomas are the good guyssmall, lipidrich, and often harmless. On a noncontrast CT they sit under 10HU, and after contrast they wash out quickly (absolute washout >60%). MRI will show signal loss on outofphase images because of that internal fat.
Carcinomas, on the other hand, are usually >10HU, have poor washout (<60%), and retain their signal on chemicalshift sequences. They may also show necrotic areas and heterogeneous enhancement.
Pheochromocytoma vs. Carcinoma (T2 Brightness & Kinetics)
Pheochromocytomas love T2theyre often called lightbulb lesions because they blaze bright on T2weighted images. They also enhance rapidly in the arterial phase. Carcinomas can look similar but usually have more irregular borders and may contain calcifications.
Myelolipoma & Other Benign Masses (Fat Content)
Myelolipomas are packed with macroscopic fat. On CT they appear very dark (30HU or lower) and on MRI they have classic fat signalso you can spot them instantly. Theyre benign, but large ones can cause pain.
Quick Reference Table
| Lesion | Key CT Feature | Key MRI Feature | Typical HU | Washout | Clinical Hint |
|---|---|---|---|---|---|
| Adenoma | Homogeneous, <10HU | Signal loss on outofphase | 10 | >60% | Incidental |
| Carcinoma | Heterogeneous, >10HU, necrosis | No signal loss, diffusion restriction | >10 | <60% | Hormone excess, rapid growth |
| Pheochromocytoma | Variable HU, avid arterial enhancement | Lightbulb T2 hyperintensity | Variable | Variable | Hypertension, catecholamines |
| Myelolipoma | Macroscopic fat (30HU) | Fat signal on both sequences | <30 | N/A | Asymptomatic |
RealWorld Experience
Case 1 EarlyStage Surprise
Jane, 42, had an abdominal CT for unrelated kidney stones. The radiologist spotted a 4cm adrenal mass that looked suspiciouswashout was only 55%. MRI confirmed no fat signal, and a biopsy revealed adrenocortical carcinoma (ACC). She underwent laparoscopic adrenalectomy and has been diseasefree for two years. This illustrates why size alone can be misleading; the imaging characteristics clinched the diagnosis.
Case 2 Advanced Disease Unveiled by PETCT
Mark, 58, presented with high blood pressure and occasional palpitations. A CT showed an 8cm adrenal tumor. PETCT lit up several lung nodules and a lytic lesion in the spineclassic adrenal metastasis radiology. The multidisciplinary team started him on neoadjuvant chemotherapy before attempting surgery. Unfortunately, his disease progressed, underscoring how vital wholebody staging is for setting realistic expectations.
These stories arent just medical anecdotes; theyre proof that the right imaging pathway can change a life trajectoryeither by catching a tumor early enough for cure or by sparing a patient from unnecessary surgery when the disease is already widespread.
Pitfalls to Avoid
Overreliance on Size Alone
Its tempting to think tiny = harmless. Small adrenal lesions can still be aggressive, especially when they show poor washout or irregular borders. Always pair size with attenuation and enhancement patterns.
Misinterpreting Washout in Necrotic Tumors
Large carcinomas often have necrotic (dead) tissue that appears lowdensity, mimicking a benign washout pattern. Crosscheck with MRI diffusion or PETCT to avoid false reassurance.
Ignoring Functional Imaging When Hormone Tests Are Positive
If labs show excess catecholamines or cortisol, a standard CT might miss a small, metabolically active lesion. In such cases, consider functional PET tracers like CMTO or FFDOPA.
TakeHome Checklist
- Order a contrastenhanced multiphase CT for any adrenal mass >1cm.
- Calculate absolute washout; <60% suggests malignancy.
- When CT is equivocal, add chemicalshift MRI to assess lipid content.
- For lesions>5cm or highgrade features, schedule a PETCT for wholebody staging.
- Document stage using the radiologic criteria tablethis guides surgery vs. systemic therapy.
- Communicate findings in a structured report: technique, measurements, impression, recommendations.
- Integrate hormone panel results; coordinate with endocrinology for functional tumors.
- Discuss every case at a multidisciplinary tumor boardradiology, surgery, oncology, pathology.
Conclusion
Staging adrenal carcinoma radiologically isnt just a series of scans; its a collaborative detective story where every image clue shapes the next chapter of care. By mastering CT washout, MRI chemicalshift, and PETCT metabolic mapping, clinicians can accurately stage the disease, avoid unnecessary procedures, and tailor treatment to each individuals situation. Realworld cases show that early, precise imaging can lead to cure, while comprehensive wholebody staging spares patients from false hope when the cancer has already spread.
Now that youve got the roadmap, youre better equipped to ask the right questions of your doctors, understand their answers, and feel more in control of your (or a loved ones) journey. If you have any doubts or want to share your own experience, drop a comment belowlets keep the conversation going. Together, we can turn daunting medical jargon into clear, actionable knowledge.
FAQs
What imaging tests are used for adrenal carcinoma staging?
The primary studies are contrast‑enhanced CT, MRI with chemical‑shift sequences, and ¹⁸F‑FDG PET‑CT for detecting distant metastases.
How does CT washout help differentiate benign from malignant adrenal lesions?
Benign adenomas typically show an absolute washout > 60 % on delayed images, whereas carcinomas have washout < 60 %, indicating less rapid contrast clearance.
When is MRI preferred over CT in adrenal cancer evaluation?
MRI is used when CT findings are inconclusive, especially to assess soft‑tissue invasion, vascular involvement, or to detect microscopic fat with out‑of‑phase imaging.
What does a PET‑CT reveal that CT or MRI might miss?
PET‑CT highlights metabolically active disease and can uncover distant metastases in the lungs, liver, bone, or brain that are not visible on anatomic scans alone.
Why is multidisciplinary discussion essential after imaging?
Radiologic stage determines whether the patient proceeds to surgery, needs neoadjuvant therapy, qualifies for clinical trials, or should receive palliative care, so input from surgeons, oncologists, endocrinologists, and radiologists is crucial.