Most people dont realize that an adrenal carcinoma can look totally different on a CT scan than a harmless adenoma and those differences are what dictate lifesaving treatment.
In the next few minutes well cut through the jargon, show you exactly how radiologists spot a malignant adrenal mass, stage it, and keep patients safe. Grab a coffee, settle in, and lets talk about adrenal carcinoma radiology together.
Why Imaging Matters
When a tumor sneaks up on the adrenal gland, the first line of defense isnt a blood test its an image. A clear picture can turn a vague incidentaloma into a concrete diagnosis, and that can be the difference between watchful waiting and urgent surgery.
What is adrenal carcinoma and how rare is it?
Adrenocortical carcinoma (ACC) is a malignant tumor arising from the cortex of the adrenal gland. It accounts for less than 0.2% of all cancers, but its aggressive nature makes early detection crucial. According to a recent , patients diagnosed at a localized stage have a fiveyear survival rate exceeding 70%, while advanced disease drops below 20%.
What does radiology actually accomplish?
Radiology does four things for ACC:
- Diagnosis: Identifies suspicious features that separate cancer from benign masses.
- Staging: Maps local invasion, lymph nodes, and distant metastases.
- Treatment planning: Guides surgeons and oncologists on the best approach.
- Followup: Monitors for recurrence after surgery or systemic therapy.
Realworld snippet
Imagine a 45yearold named Maya who went in for a routine abdominal CT after a mild back ache. The scan showed a 3.5cm adrenal nodule that looked benign at first glance. A careful review of the contrast washout curves revealed a low washout a red flag for ACC. Within weeks, Mayas tumor was removed surgically, and shes now cancerfree. That single image changed everything.
Core Imaging Modalities
| Modality | Typical Findings in ACC | Key Advantage | Pitfall to Watch |
|---|---|---|---|
| CT Scan | Heterogeneous enhancement, necrosis, low absolute washout | Widely available, excellent spatial resolution | Radiation dose; relies on timing for washout accuracy |
| MRI | Mixed T1/T2 signal, diffusion restriction, lack of chemical shift loss | No ionizing radiation; superior softtissue contrast | Longer exam time; gadolinium contraindications |
| PET/CT | High FDG uptake (SUV>34), helps detect distant metastasis | Functional information; wholebody staging | Expensive; false positives in inflammatory lesions |
| Ultrasound | Limited; may show hypoechoic mass in thin patients | Bedside, no radiation | Operator dependent; poor visualization of deep adrenal glands |
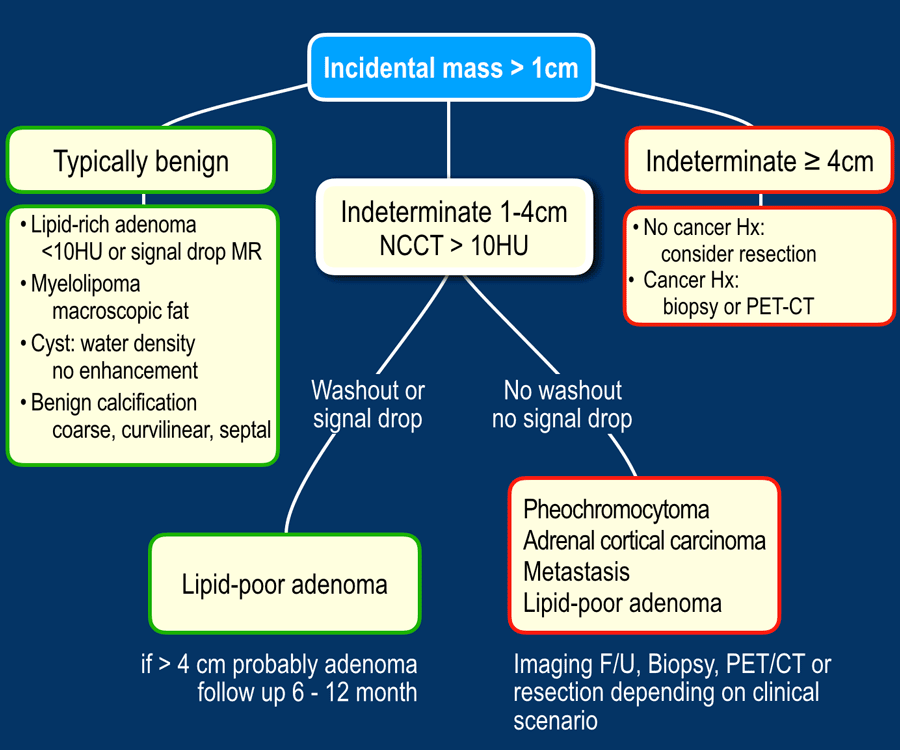
CT Scan contrast washout patterns
CT is the workhorse for adrenal evaluation. After a rapid iodinated contrast bolus, radiologists measure the attenuation (in Hounsfield units) of the lesion at 1015 minutes. An absolute washout60% or a relative washout40% usually points to a benign adenoma. ACC tends to retain contrast, showing low washout thats the hallmark of adrenal washout radiology.
MRI chemical shift and diffusion
On inphase versus outofphase images, a benign adrenal adenoma loses signal (the chemical shift effect) because of microscopic fat. ACC, lacking this intracellular fat, retains its signal. Adding diffusionweighted imaging (DWI) helps: ACC often shows restricted diffusion, appearing bright on highbvalues and dark on apparent diffusion coefficient maps.
PET/CT spotting metastasis
FDGPET is especially useful when the disease spreads beyond the adrenal gland. High glucose metabolism lights up the tumor and any distant sites, such as lungs, bone, or brain. According to the , PET/CT is the recommended tool for detecting metastatic adrenal carcinoma.
Differentiating Common Lesions
Adrenal adenoma radiology
Benign adenomas are usually small (<4cm), homogeneous, and demonstrate rapid contrast washout. On MRI, the chemical shift loss is obvious, and they often have low attenuation (<10 HU) on noncontrast CT.
Pheochromocytoma radiology
Pheochromocytomas are catecholamineproducing tumors that love to be bright on T2 (lightbulb sign) and show avid enhancement after contrast. Unlike ACC, they rarely have necrotic areas and tend to be more vascular.
Adrenal myelolipoma radiology
These benign lesions contain macroscopic fat, so on CT they appear very low density (80 to120 HU). MRI confirms fat with high signal on both T1 and T2, and fatsuppressed sequences will make them disappear.
Adrenal metastasis radiology
When another primary cancer spreads to the adrenal, the lesions are often bilateral, heterogeneous, and may have a known primary on imaging. They typically lack the rapid washout of adenomas and dont exhibit the bright T2 signal of pheochromocytoma.
Comparison Table
| Feature | ACC | Adenoma | Pheochromocytoma | Myelolipoma |
|---|---|---|---|---|
| Size | >4cm common | <4cm | Variable | Variable |
| Washout | Low | High | Intermediate | N/A (fat) |
| HU (noncontrast) | >30 | <10 | 3050 | 80to120 |
| T2 signal | Mixed | Lowmoderate | Very high | High (fat) |
| Necrosis | Common | Rare | Rare | Absent |
Staging the Disease
Local invasion
CT and MRI can reveal whether ACC has breached the renal vein, inferior vena cava, liver, or pancreas. Loss of the fat plane between the adrenal gland and adjacent organs is a warning sign. Radiologists also look for direct tumor extension into the perinephric fat or diaphragmatic crus.
Lymph node assessment
Enlarged paraaortic or hilar nodes (>1cm short axis) raise suspicion, but size alone is not definitive. Morphology round shape, loss of fatty hilum, and necrotic center adds confidence.
Distant metastasis
The most common sites for ACC spread are the lungs, liver, bone, and brain. A chest CT screens for pulmonary nodules, while a bone scan or FDGPET picks up skeletal lesions. MRI is preferred for brain surveillance.
Case Study
John, 60, presented with vague abdominal pain. Imaging showed a 9cm right adrenal mass invading the IVC, enlarged paraaortic nodes, and multiple lung nodules on chest CT. The radiology report staged his disease as StageIV ACC, prompting systemic therapy before any surgical attempt. Within six months, repeat PET/CT showed a good metabolic response, underscoring the power of accurate staging.
Reporting Standards Checklist
Structured reporting template
Consistency helps both radiologists and clinicians. A good report includes:
- Lesion size (max diameter in three planes)
- Margins (smooth, lobulated, infiltrative)
- Attenuation values (HU) on noncontrast and postcontrast phases
- Washout percentages (absolute & relative)
- Necrosis, hemorrhage, calcification
- Evidence of local invasion (vascular, organ)
- Regional lymph node status
- Presence of distant metastasis
When to recommend a biopsy
Guidelines suggest biopsy only when imaging is indeterminate and the result would change management. For example, a lesion with ambiguous washout that could be either ACC or a pheochromocytoma might need tissue confirmation, especially if the patient is not a surgical candidate.
Communicating risk to patients
We balance the benefits of early detection with the risks of radiation, contrast reactions, and anxiety from false positives. Using visual aidsannotated images that highlight suspicious areashelps patients understand why a test is recommended and what the possible outcomes are.
Expert tip
Always pair imaging findings with hormonal workup. A functional tumor (e.g., excess cortisol or catecholamines) reinforces the suspicion raised by radiology.
RealWorld Experiences
Janes story
Jane, 38, had an incidental 2.5cm adrenal nodule discovered during a CT for kidney stones. The radiologist noted a borderline washout (45%) and sent it for a dedicated adrenal protocol. The followup MRI revealed heterogeneous T2 signal and restricted diffusion. The multidisciplinary team opted for laparoscopic adrenalectomy, and pathology confirmed a lowgrade ACC. Janes case illustrates how a small, seemingly innocuous nodule can hide a malignancy that imaging catches early.
Radiologist insight
When I see a large, heterogeneous adrenal mass with low washout, I immediately think ACC, says Dr. Alvarez, a boardcertified abdominal radiologist with 15years of experience. But I never rely on imaging alone; I always correlate with clinical signs and labs. That synergy is what turns a guess into a diagnosis.
Lesson learned
Integrating imaging with hormonal assays and patient history is the gold standard for accurate diagnosis.
Balancing Benefits & Risks
Benefits of highresolution imaging
Accurate imaging guides surgeons to the right operative plan, can spare patients unnecessary surgeries, and detects metastasis early, which opens doors to targeted therapies. For patients facing cancers elsewhere (for example, renal masses), coordinating imaging and nutrition planning is often part of a broader care plan that includes discussions about Renal cancer nutrition alongside staging.
Risks you should know
CT delivers ionizing radiation, which matters especially for younger patients. Iodinated contrast can strain kidneys, and gadoliniumbased agents have rare but serious side effects. Falsepositive findings may cause anxiety and lead to invasive procedures.
Mitigation strategies
- Use lowdose CT protocols for followup scans.
- Prefer MRI when radiation is a concern, especially in children or pregnant patients.
- Employ noncontrast sequences and chemical shift imaging to reduce unnecessary contrast use.
- Discuss the riskbenefit ratio openly with patients, fostering shared decisionmaking.
Conclusion
Adrenal carcinoma radiology hinges on recognizing heterogeneous enhancement, low contrast washout, and the full staging picture on CT or MRI. By pairing expert image interpretation with clear communication, clinicians can navigate the fine line between overtesting and missing a lifethreatening tumor. If you or a loved one faces an adrenal mass, ask your radiologist for a detailed, structured report, stay updated with the latest guidelines, and never hesitate to discuss the findings with your care team. Knowledge is power, and in the world of adrenal imaging, it truly saves lives.
FAQs
What imaging modality is preferred for initial evaluation of adrenal carcinoma?
CT scan is the primary imaging modality for adrenal carcinoma evaluation due to its wide availability and excellent spatial resolution, allowing detection of heterogeneous enhancement, necrosis, and washout patterns critical for diagnosis.
How does adrenal carcinoma typically appear on CT imaging?
Adrenal carcinoma usually appears as a large (>4 cm), heterogeneous mass with irregular margins, areas of necrosis, and low absolute and relative contrast washout on CT scans.
What is the role of MRI in adrenal carcinoma radiology?
MRI provides superior soft tissue contrast without ionizing radiation, showing mixed T1/T2 signals, restricted diffusion on diffusion-weighted imaging, and no chemical shift signal loss, helping differentiate carcinoma from benign lesions.
When is PET/CT recommended in adrenal carcinoma cases?
PET/CT is mainly used for whole-body staging to detect distant metastases in lungs, liver, bone, and brain due to high FDG uptake in malignant lesions, enhancing treatment planning.
How do radiologists differentiate adrenal carcinoma from adenoma on imaging?
The key differences include larger size (>4 cm), heterogeneous enhancement, low contrast washout in carcinoma versus small size (<4 cm), homogeneous appearance, and high contrast washout in adenomas, along with differences in Hounsfield units and MRI chemical shift effects.