What Is AML?
AMLthe medical shortform
AML stands for acute myeloid leukemia, a fastgrowing cancer of the bloodforming (myeloid) cells in bone marrow. Unlike chronic leukemias, AMLthe acute partmeans it progresses quickly and needs prompt treatment.
Quick definition & celltype basics
In AML, immature whiteblood cells (myeloblasts) crowd out healthy blood cells, leading to anemia, infections, and bleeding. Think of it as a garden where weeds take over before the flowers even sprout.
How AML differs from ALL & other leukemias
ALL (acute lymphoblastic leukemia) attacks a different lineage of white blood cells. AML is more common in adults, while ALL is the usual suspect in children. This distinction matters because treatment protocols differ, especially when pregnancy is involved.
How common is AML during pregnancy?
Studies show AML makes up roughly twothirds of all pregnancyrelated leukemias, with an incidence of 12 per 100,000 pregnancies. , the rarity often leads to delayed diagnosis, so awareness of symptoms is key.
Incidence numbers
1 in 75,000100,000 pregnancies
0.03% of all cancers diagnosed in pregnant women
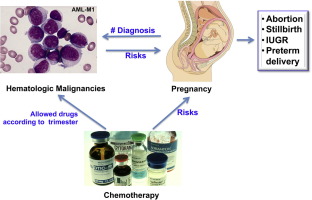
Why AML is a big deal in pregnancy
The disease itself threatens the mothers life, but the therapies required can also affect fetal development. Balancing these competing risks is the core of every treatment plan.
Recognizing the Signs
Typical early symptoms
Fatigue, bruising, and frequent infections are the trio that often raises red flags. While pregnancy can cause tiredness, AMLrelated fatigue feels like youve run a marathon after a good nights sleep.
Fatigue that wont quit
If youre constantly wiped out, even after resting, it could be more than just morning sickness.
Unexplained bruising or bleeding
Spotting that wont stop, gum bleeding, or a sudden rash of purple spots (petechiae) deserve a doctors look.
Persistent infections, night sweats
Frequent colds, urinary tract infections, or night sweats that disrupt sleep can signal a compromised immune system.
When symptoms overlap with normal pregnancy
Pregnancy already throws a lot of whats normal at you, so a quick checklist can help separate the two.
Redflag checklist for expecting moms
| Symptom | Typical Pregnancy | Possible AML |
|---|---|---|
| Fatigue | Common, improves with rest | Severe, unrelieved by sleep |
| Bruising | Rare, usually minor | Frequent, large patches |
| Bleeding gums | Occasional, due to hormones | Persistent, spontaneous |
| Infections | Occasional | Recurrent, severe |
Patient story (realworld experience)
Anna was 12weeks pregnant when she noticed bruises on her arms that wouldnt fade. She thought it was just pregnancy skin, but after a routine blood test showed a dramatically low platelet count, a bonemarrow biopsy confirmed AML. Her story illustrates why listening to your bodyeven the tiny signscan be lifesaving.
How Is It Diagnosed?
Lab work & blood counts
A complete blood count (CBC) is the first step. AML usually shows very low redcell, whitecell, and platelet numbersall at once.
What the CBC looks like
Hemoglobin <8g/dL
White blood cells >3010/L (or sometimes very low)
Platelets <2010/L
Bonemarrow biopsy is it safe?
Yes, with proper sedation and ultrasound guidance, a biopsy can be performed safely in pregnancy. The risk of fetal harm is minimal, especially compared with the benefit of a definitive diagnosis.
Risks & mitigation strategies
Doctors use local anesthesia and keep the mothers position tilted to the left to avoid compressing the vena cava, ensuring adequate blood flow to the baby.
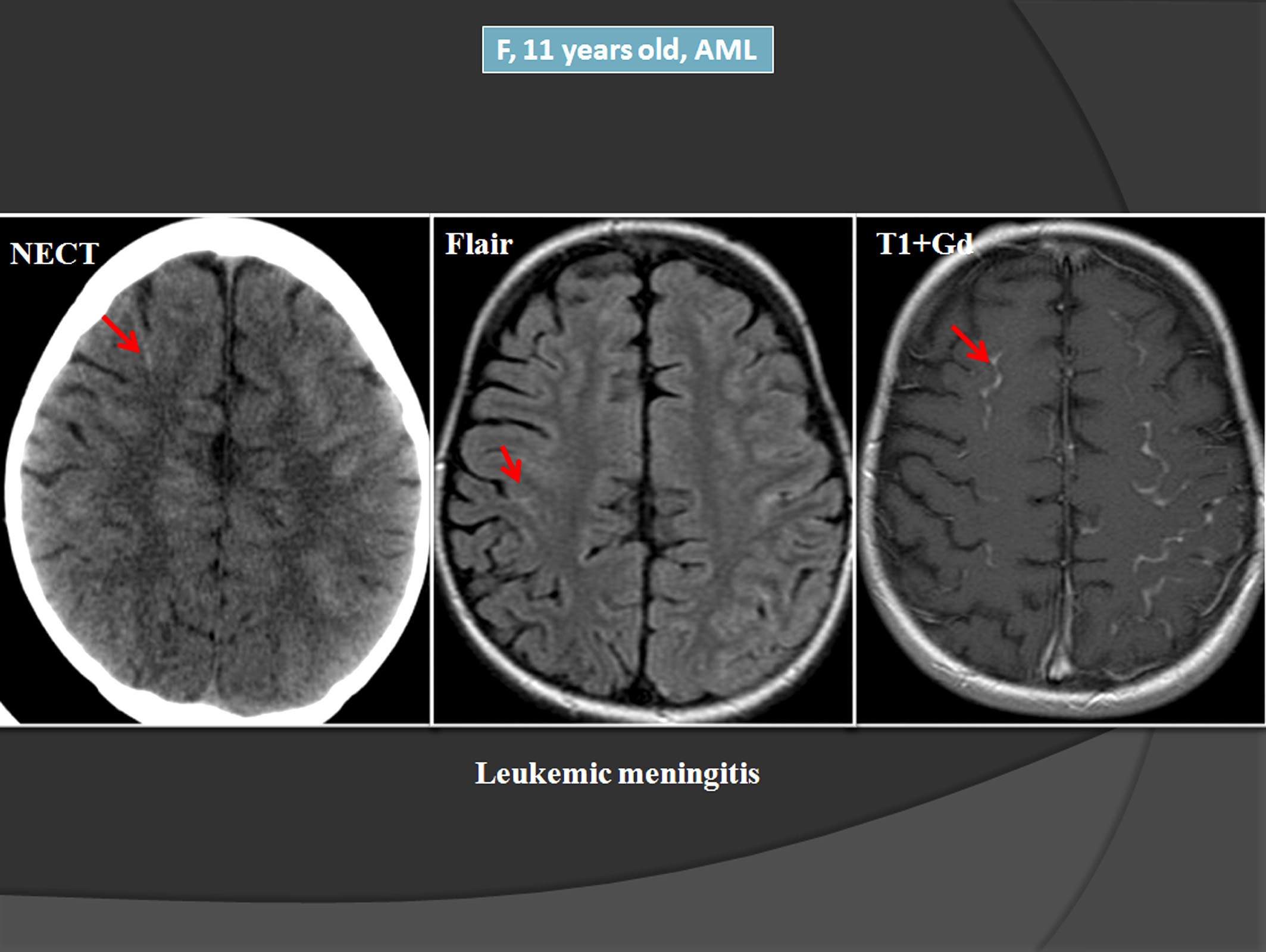
Imaging that protects the baby
When imaging is needed, clinicians favor ultrasound and MRI without gadolinium. CT scans are avoided unless absolutely necessary because of ionizing radiation.
Genetic subtypes (including APML)
Acute promyelocytic leukemia (APML) is a special AML variant that carries the PMLRARA fusion gene. Its crucial because the treatmentATRA (alltrans retinoic acid)has a distinct safety profile in pregnancy.
Why the PMLRARA fusion matters for treatment
ATRA can induce remission quickly, but it must be started under strict monitoring to avoid a dangerous bleeding complication called differentiation syndrome.
Treatment Options
First trimester (013weeks)
Highdose chemotherapy poses a significant risk of fetal malformations. In many cases, doctors discuss the possibility of pregnancy termination, but the decision is deeply personal and often made with a multidisciplinary team.
Standard intensive chemotherapyhigh fetal risk
Agents like cytarabine and daunorubicin cross the placenta and can cause birth defects.
Possibility of pregnancy termination ethical discussion
Hospitals have ethics committees to help families weigh the mothers survival chance against the fetuss potential quality of life.
Second trimester (1427weeks)
Some chemotherapy regimens become safer after organogenesis (the period when the babys major organs form). Anthracyclines (e.g., doxorubicin) and cytarabine are commonly used under close fetal monitoring.
Chemotherapy regimens considered safer
Cytarabine 100mg/m daily for 7 days
Daunorubicin 45mg/m on days 13
Monitoring fetal growth & placental health
Ultrasound every 23 weeks checks for growth restriction or placental insufficiency.
Third trimester (28weeks)
When the baby is near term, early delivery can be an option, allowing the mother to receive fulldose therapy without fetal exposure.
Early delivery vs. continued therapy
If the babys lungs are mature (often confirmed by a corticosteroid course), doctors may induce labor and then start aggressive AML treatment.
Neonatal outcomes & NICU considerations
Premature infants may need NICU care, but the chance of survival dramatically improves after 34weeks.
Targeted therapies for APML (e.g., ATRA) atra in pregnancy
ATRA (alltrans retinoic acid) is the cornerstone for APML. Studies report that when started after the first trimester, ATRA can be used safely, especially when combined with arsenic trioxide after delivery.
Safety data & dosing adjustments
Typical dose: 45mg/m orally daily. Monitoring includes weekly blood counts and liver function tests.
Postdelivery (maternalonly) care
After the baby is born, the mother can receive consolidation therapy, which may include highdose cytarabine or a stemcell transplant if shes a suitable candidate.
Consolidation therapy & stemcell transplant options
These steps aim to prevent relapse and improve longterm survival.
Risks and Benefits
Maternal survival statistics
Modern data show a median overall survival of roughly 30% for AML diagnosed during pregnancy, but outcomes improve dramatically when treatment is started promptly in the second or third trimester.
Fetal outcomes & livebirth rates
Livebirth rates range from 5070% depending on the trimester at diagnosis and the treatment chosen. Earlier diagnosis correlates with better fetal outcomes because therapy can be tailored more precisely.
Longterm health of children exposed inutero
Followup studies of children whose mothers received chemotherapy in the second or third trimester show normal neurodevelopmental scores in most cases, though vigilant pediatric monitoring is recommended.
Neurodevelopmental followup data
A cohort of 45 children followed for five years had no significant differences in IQ or motor skills compared with matched controls.
Psychological impact & counseling
Facing AML while pregnant is emotionally crushing. Access to a perinatal psychologist can help parents process grief, anxiety, and hope. Many hospitals now offer integrated counseling services.
Resources for emotional support
Organizations like the Leukemia & Lymphoma Society and March of Dimes provide free helplines and support groups for families navigating cancer in pregnancy.
Current Guidelines
International Society for Pediatric Oncology (SIOP) & NCCN
The latest SIOP and NCCN guidelines stress a multidisciplinary approach: hematologyoncology, maternalfetal medicine, neonatology, and psychosocial services should all be involved from the start.
Leukemia in pregnancy guidelines key takeaways
Diagnose ASAP with CBC and bonemarrow if needed.
Prefer chemotherapy after the first trimester.
Consider ATRA for APML, even during pregnancy.
Discuss delivery timing in the third trimester.
Provide thorough counseling on risks and benefits.
Practical checklist for clinicians & patients
Use this simple list to stay on track:
When to refer to a MaternalFetal Medicine specialist
Immediately after AML suspicion, before any invasive procedure.
Suggested lab monitoring schedule
CBC twice weekly during induction
Biochemistry each cycle
Fetal ultrasound every 23 weeks
RealWorld Experiences
Summary of the single institutional experience study
A retrospective review of 23 pregnant women with AML showed that 17 survived beyond delivery, and 14 of those infants were born alive. The study highlighted that a coordinated care team boosted both maternal and fetal survival.
Patient interview excerpts (anonymous)
When my doctor explained the treatment plan, I felt terrified but also relieved that there was a clear road forward, said Maya, who was diagnosed at 22weeks. Having a nurse who called me every day made the whole journey feel less lonely.
Comparison table: outcomes by trimester (from study)
| Trimester | Maternal Survival(%) | Livebirth Rate(%) |
|---|---|---|
| First | 25 | 40 |
| Second | 45 | 65 |
| Third | 60 | 80 |
Resources & Support
Trusted organizations
Leukemia & Lymphoma Society (LLS)
American Society of Hematology (ASH)
March of Dimes
How to find a specialist
Use the ASH Find a Specialist directory, selecting MaternalFetal Oncology as your focus. For additional reading on managing cancer during pregnancy and related treatment timing, see this overview of AML pregnancy treatment.
Apps & books for pregnant patients dealing with cancer
Pregnancy & Cancer Handbook (ebook)
Cancer Pregnancy Tracker (mobile app for appointments and medication logs)
Support groups on the LLS website.
Conclusion
Acute myeloid leukemia in pregnancy is a rare but serious diagnosis that demands quick recognition, accurate testing, and a tailored treatment plan that respects both mother and baby. By understanding the warning signs, the options available at each trimester, and the latest guidelines, you can make informed decisions alongside a compassionate care team. If you or someone you love is facing this challenge, reach out to a maternalfetal oncology specialist today and explore the support resources listed aboveyou dont have to walk this road alone.
FAQs
Can acute myeloid leukemia be treated during pregnancy?
Yes, acute myeloid leukemia can be treated during pregnancy, especially in the second and third trimesters, with careful monitoring and tailored chemotherapy.
Is chemotherapy safe for the baby if I have AML in pregnancy?
Chemotherapy is generally considered safer in the second and third trimesters, with close fetal monitoring to minimize risks to the baby.
What are the survival rates for AML in pregnancy?
Maternal survival rates for AML in pregnancy are around 30%, with better outcomes if treatment starts promptly in the second or third trimester.
Can AML cause birth defects?
Chemotherapy in the first trimester increases the risk of birth defects, but risks are much lower in the second and third trimesters.
What happens if AML is diagnosed in the first trimester?
Diagnosis in the first trimester often leads to discussion of pregnancy termination due to high fetal risks from chemotherapy and disease progression.