Acute lymphoblastic leukemia (ALL) is a fastgrowing blood cancer that starts in the bone marrow and sends a wave of immature whiteblood cells into the bloodstream. In the next few minutes youll get straighttothepoint answers about what it feels like, how doctors spot it, what treatments exist for kids and adults, and what the survival numbers really mean.
What Is ALL
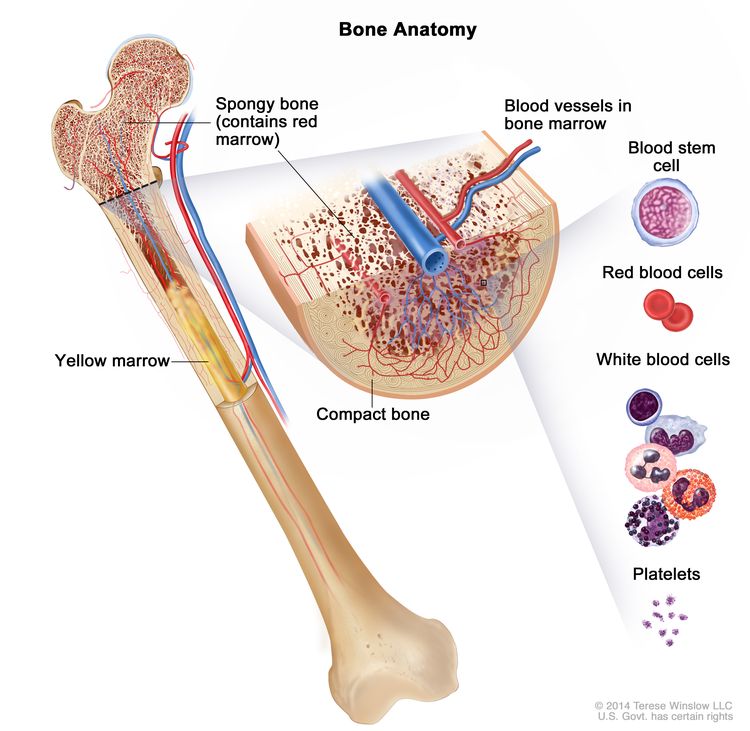
How does ALL develop in the bone marrow?
In a healthy marrow, stem cells mature into different blood cells that keep our bodies running. With ALL, a genetic mutation (often in the TCL1, NOTCH1, or Philadelphia chromosome genes) hijacks a lymphoid precursor, forcing it to multiply without maturing. The result? A crowd of blast cells that crowd out red cells, platelets, and normal white cells.
These blasts spill into the bloodstream, causing the classic symptoms well talk about later. For a deeper dive into the biology, the offers a clear, peerreviewed explanation.
Key differences between ALL and other leukemias
| Feature | ALL | AML (Acute Myeloid Leukemia) | CLL (Chronic Lymphocytic Leukemia) |
|---|---|---|---|
| Cell line | Lymphoid (B or Tcell) | Myeloid | Mature Bcells |
| Onset speed | Very rapid | Rapid | Slow, often incidental |
| Typical age | Children (25yr) & young adults | Adults >60yr | Adults >60yr |
| Treatment intensity | Highdose chemo targeted therapy | Highdose chemo transplant | Watchful waiting or gentle therapy |
Who Gets ALL
Acute lymphoblastic leukemia in children
Kids are the most common group. In the United States, about 3,000 new pediatric cases appear each year, with the highest incidence between ages 2 and 5. The disease is slightly more common in boys, and certain genetic syndromes (like Down syndrome) increase risk.
Imagine a parents voice trembling on a phone call: Were waiting for the results I just want to know theres hope. That hope is realthanks to decades of research, the 5year survival for children now exceeds 85% in highresource settings ().
Acute lymphoblastic leukemia in adults
Adults account for roughly 20% of ALL cases. The average age at diagnosis is 39, but theres a second bump in people over 60. Unlike kids, adults often face more aggressive disease biology, lower tolerance for intense chemotherapy, and unfortunately lower survival ratesaround 4050% 5year overall survival.
One adult patient, Mark, told his oncologist, I thought leukemia only happened to kids. I feel like Im starting over at 45. Stories like Marks remind us that awareness across ages is crucial.
Rare cases & special populations
Infants (<1yr) can have a distinct, highrisk form driven by MLL gene rearrangements. The elderly (>70yr) may face comorbidities that limit treatment options. In each scenario, a personalized approachbalancing treatment benefit with quality of lifeis essential.
Spotting Warning Signs
Most common acute lymphoblastic leukemia symptoms
- Persistent fatigue or weakness
- Easy bruising or unexplained bleeding
- Fever that wont go away
- Bone or joint pain (often in the long bones)
- Swollen lymph nodes, especially in the neck or armpits
- Frequent infections (colds, sinusitis, pneumonia)
These symptoms overlap with many everyday ailments, which is why many families dismiss them as just a bad flu. But when they appear together or worsen quickly, its worth a doctors visit.
When symptoms differ between kids & adults
| Age Group | Typical First Symptom | Common Additional Clues |
|---|---|---|
| Children | Bone pain or limp | Night sweats, pale skin, swollen gums |
| Adults | Unexplained fatigue | Weight loss, night fevers, recurrent infections |
Red flags that demand immediate medical attention
If you notice sudden swelling of the abdomen, severe shortness of breath, or uncontrolled bleeding, call emergency services. These could signal a rapid rise in blast cells that threatens organ function.
How Is Diagnosed
Blood work & what it reveals
A complete blood count (CBC) often shows low red blood cells (anemia), low platelets (thrombocytopenia), and a high whitecell count with a significant proportion of blasts. The blast percentage is the primary screening flag.
Bonemarrow biopsy the gold standard
During a short, outpatient procedure, a needle extracts a small marrow sample from the hip bone. Pathologists examine it under a microscope to confirm >20% blasts, which officially defines ALL. While the idea may sound scary, most patients report only mild discomfort and a quick recovery.
Cytogenetics & molecular testing
Modern labs run fluorescence insitu hybridization (FISH) and nextgeneration sequencing to detect specific genetic changeslike the Philadelphia chromosome (BCRABL1), which alters treatment options dramatically. Detecting these alterations early can open the door to targeted therapies that spare patients from unnecessarily harsh chemotherapy.
Staging & risk stratification
Doctors classify ALL into standard, high, or very high risk based on age, whitecell count at diagnosis, and genetic features. This classification decides how aggressive the treatment will be and helps predict prognosis.
Treatment Options
Standard chemotherapy protocols
Most patients start with a multiphase regimen: induction (to achieve remission), consolidation (to eliminate residual disease), and maintenance (to keep the disease at bay for years). Common drugs include vincristine, prednisone, anthracyclines, and Lasparaginase.
Targeted & immunotherapy breakthroughs
When a Philadelphia chromosome is present, adding a tyrosinekinase inhibitor like imatinib dramatically improves outcomes. For relapsed or refractory disease, CART cell therapywhere a patients own Tcells are engineered to hunt leukemia cellshas shown remission rates above 80% in some trials.
Treatment differences: children vs. adults
Kids usually tolerate higherdose chemotherapy and have protocols that span 23years, often with less longterm organ damage. Adults, especially older ones, may receive lowerintensity regimens combined with targeted agents to balance efficacy and toxicity.
Clinical trial participation why its worth discussing
New drugs and combinations emerge every year. Enrolling in a trial can give patients access to cuttingedge therapies while contributing to scientific knowledge. The maintains a searchable database of active ALL trials.
Prognosis & Survival
Acute lymphoblastic leukemia survival rate
Overall, the 5year survival across all ages hovers around 60%. Breaking it down:
- Children: >85% (in highresource settings)
- Adolescents/young adults: 7080%
- Adults >40% (improving with targeted therapies)
Factors that improve outlook
Age under 20, a normal whitecell count at diagnosis, the absence of highrisk genetic mutations, and rapid achievement of minimal residual disease (MRD) negativity are all linked with better survival. Simply put, the sooner the disease is caught and the more precisely its treated, the brighter the odds.
Longterm followup & survivorship care
Even after remission, survivors need regular monitoring for late effectslike heart problems from anthracyclines, hormonal changes, or secondary cancers. Support groups, counseling, and a coordinated care team help maintain both physical health and emotional wellbeing.
Living With ALL
Managing side effects at home
Chemo can bring nausea, fatigue, and hair loss. Small, practical stepslike sipping ginger tea for nausea, eating frequent small meals, and using a soft-bristled toothbrush for a sore mouthcan make a big difference. Hydration is key; aim for at least 8 glasses of water daily.
Psychological coping strategies
Facing a cancer diagnosis is an emotional rollercoaster. Journaling, mindfulness apps, and talking with a therapist can help process feelings. Many families find comfort in connecting with others who have walked the same roadonline forums hosted by the are bustling with shared stories and tips.
Trusted organizations & where to find help
Beyond the LLS, the offers free counseling hotlines, while the provides indepth patient guides you can download. For patients concerned about pregnancy and leukemia treatment options, information about leukemia pregnancy treatment can be an important resource when planning care that balances maternal and fetal health.
Conclusion
Acute lymphoblastic leukemia is a serious, fastacting blood cancer, but understanding its signs, getting diagnosed early, and accessing modern therapies can dramatically improve outcomes. Whether youre a parent, a patient, or a supportive friend, staying informed, leaning on expert care, and embracing a strong support network are the best ways to navigate this journey. If you have questions, personal stories, or need a listening ear, feel free to share them in the commentstogether were stronger.
FAQs
What are the most common early symptoms of acute lymphoblastic leukemia?
Typical early signs include persistent fatigue, easy bruising or bleeding, bone or joint pain (often in the long bones), fever that doesn’t resolve, and frequent infections.
How do doctors confirm a diagnosis of ALL?
Diagnosis begins with a complete blood count that shows abnormal red cells, platelets, and blasts. Definitive confirmation requires a bone‑marrow biopsy showing ≥20 % lymphoblasts, followed by cytogenetic and molecular testing (FISH, PCR, or next‑generation sequencing) to identify specific genetic abnormalities.
What treatment approaches are used for children with ALL?
Children usually receive multi‑phase chemotherapy (induction, consolidation, maintenance) that may include vincristine, prednisone, anthracyclines, and L‑asparaginase. High‑risk patients may also get targeted agents (e.g., tyrosine‑kinase inhibitors for Ph‑positive disease) or participate in clinical trials offering novel immunotherapies.
How does the Philadelphia chromosome influence therapy decisions?
The presence of the BCR‑ABL1 fusion (Philadelphia chromosome) makes the leukemia sensitive to tyrosine‑kinase inhibitors such as imatinib, dasatinib, or ponatinib. Adding a TKI to standard chemotherapy greatly improves remission rates and long‑term survival compared with chemotherapy alone.
What long‑term follow‑up care do ALL survivors need?
Survivors require regular monitoring for late effects such as cardiac toxicity from anthracyclines, endocrine disorders, secondary malignancies, and neurocognitive issues. A survivorship care plan that includes periodic blood work, imaging, and supportive‑care services helps maintain health and quality of life.