Looking for the nittygritty of the ACR ankylosing spondylitis guidelines? Heres the short answer: the American College of Rheumatology (ACR) has laid out a stepbystep, evidencebased road map for diagnosing and treating both radiographic and nonradiographic axial spondyloarthritis. In the next few minutes youll get a clear picture of the key recommendations, how they compare with the EULAR and ASAS guidance, and practical tips you can start using today.
Ready? Lets dive in Ill keep things friendly, practical, and, hopefully, a little entertaining.
Guideline Overview
The ACR guideline is a comprehensive document that covers everything from who qualifies for a diagnosis to which medicines are worth trying first. It was crafted by a multidisciplinary panel that includes rheumatologists, physiotherapists, patient advocates, and methodologists, all working together to sift through the latest research and grade the evidence.
Why does this matter? Because the guideline bridges the gap between scientific trials and the everyday clinic. It tells you not just what works but when it works best, making it a reliable compass when youre navigating a complex disease like ankylosing spondylitis (AS).
For those who love the details, the full walks you through the development process, conflictofinterest safeguards, and the grading system that underpins each recommendation.
Who created the guideline?
The panel was led by boardcertified rheumatologists with decades of AS experience, plus epidemiologists who ensure the data are solid, and patient representatives who keep the language grounded in realworld concerns.
Expert insight to consider
If you have a rheumatology colleague, ask them what they think about the conditional wording for biologics that tiny nuance often sparks the most lively discussions.
Diagnosis Recommendations
Getting the diagnosis right is half the battle. The ACR guideline leans heavily on the ASAS (Assessment of SpondyloArthritis international Society) classification criteria, often called the asas criteria for ankylosing spondylitis. Those criteria are the backbone of both the ACR and the EULAR (European League Against Rheumatism) guidelines, but the ACR adds a few practical tweaks.
When should I suspect nonradiographic vs. radiographic disease?
Think of nonradiographic axial spondyloarthritis (nraxSpA) as the younger sibling of classic AS the symptoms are there, the inflammation is there, but the Xray hasnt caught up yet. If a patient has chronic back pain that improves with exercise,plus a positive HLAB27 or elevated CRP, the ACR suggests jumping straight to MRI.
What imaging modality is firstline for suspected AS?
The guideline says: start with plain radiographs of the sacroiliac (SI) joints if the pain has been lingering for more than three years. If the Xray is inconclusive and clinical suspicion remains high, order an MRI its the gold standard for early inflammation.
Imaging comparison
| Feature | ACR guideline | ASASEULAR 2022 | Key difference |
|---|---|---|---|
| First imaging | MRI of SI joints if clinical suspicion high | MRI if symptoms <3yr | ACR stresses MRI only after clinical flags |
| HLAB27 testing | Recommended when diagnosis unclear | Optional | ACR leans toward routine testing |
Realworld vignette
Emily, 28, came in with a sixmonth history of dull lowerback pain that eased after a morning stretch. Her primary doctor ordered an Xray that looked normal, but the ACR guideline nudged her rheumatologist to ask about night pain and family history. A quick MRI revealed bonemarrow edema in the SI joints confirming nraxSpA and sparing her months of trialanderror NSAID use.
Treatment Pillars
Now that we have a diagnosis, whats the game plan? The ACR frames treatment in four clear pillars: NSAIDs, supervised physical therapy, biologic or targetedsynthetic DMARDs, and a statement that conventional DMARDs (like methotrexate) arent useful for axial disease alone.
When should I switch from NSAIDs to a biologic?
If pain persists after four weeks of fulldose NSAIDs, CRP stays elevated, or imaging shows progression, the guideline recommends a conditional move to a tumornecrosis factor (TNF) inhibitor. Think of it as the nextlevel tool when firstline options stop delivering relief.
What are the main safety concerns?
Every medication has a flip side. For NSAIDs, watch for gastrointestinal bleeding and kidney issues. For biologics, the biggest red flags are infections (especially tuberculosis), possible reactivation of hepatitis B, and rare cardiovascular events. The ACR stresses prescreening and regular monitoring a small price for peace of mind.
Quickreference flowchart (text version)
- Start with NSAID+physical therapy.
- Reevaluate at 46weeks:
- If active disease (BASDAI4, CRP>5mg/L, or MRI inflammation) consider TNF inhibitor.
- If partial response doseadjust NSAID, add sulfasalazine (only if peripheral arthritis present).
- If TNF fails or contraindicated switch to IL17 inhibitor (secukinumab or ixekizumab).
- Throughout monitor labs every 3months, repeat imaging annually.
Sideeffect checklist for patients
- Fever, chills, or persistent cough? Call your doctor could be infection.
- Stomach pain or black stools? Stop NSAIDs and seek evaluation.
- New skin rash or joint swelling? Mention it; it might signal a reaction.
Guideline Differences
Its easy to think all guidelines say the same thing, but subtle divergences can shape treatment choices. The EULAR 2022 guideline, for instance, places a stronger emphasis on early MRI for all suspicious cases, while the ACR leans on clinical judgment before ordering costly scans.
Which guideline should I follow in a community clinic?
If youre in a resourcelimited setting, the ACRs tiered approach (clinical signs targeted imaging) can keep costs down without sacrificing accuracy. In a tertiary center with ready MRI access, the EULAR strategy might feel more natural.
Are there conflicts between ACR & EULAR recommendations?
Mostly, they harmonize. The biggest clash is timing: EULAR suggests MRI within three months of symptom onset, whereas ACR recommends waiting for a high clinical suspicion flag. In practice, many clinicians blend the two ordering an MRI early if the patients pain is disabling.
Top5 differences at a glance
- Imaging trigger: ACR clinical flag; EULAR symptom duration.
- NSAID dosing: ACR endorses maximum approved dose; EULAR prefers lowest effective dose.
- Biologic sequencing: ACR permits IL17 as first biologic; EULAR prefers TNF first.
- Physical therapy prescription: Both emphasize, but ACR specifies supervised programs.
- Screening for TB: Identical both require IGRA or skin test before biologics.
Practical Application
Guidelines are great on paper, but how do they translate into a realworld office visit? The secret sauce is shared decisionmaking. Talk openly about the benefits and risks, use visual aids, and document your rationale this not only builds trust but also satisfies audit requirements.
Sample 12month management plan
- Month0: Diagnosis confirmed, NSAID started, physiotherapy referral.
- Month3: Reevaluate BASDAI, CRP. If still active initiate TNF inhibitor.
- Month6: Assess response; consider dose taper if remission (BASDAI<2).
- Month12: Full review: labs, repeat MRI if progression suspected, discuss longterm biologic strategy.
How to document guideline adherence for audits?
Keep a simple checklist in the EMR: diagnosis date, criteria met (ASAS/ACR), firstline NSAID dose, PT referral, screening labs, biologic start date, and followup outcomes. This onepage snapshot satisfies most qualityimprovement reviews.
Printable clinician checklist (PDF)
Downloadable directly from the ACR site it includes boxes for each recommendation and space for notes.
Recent Advances
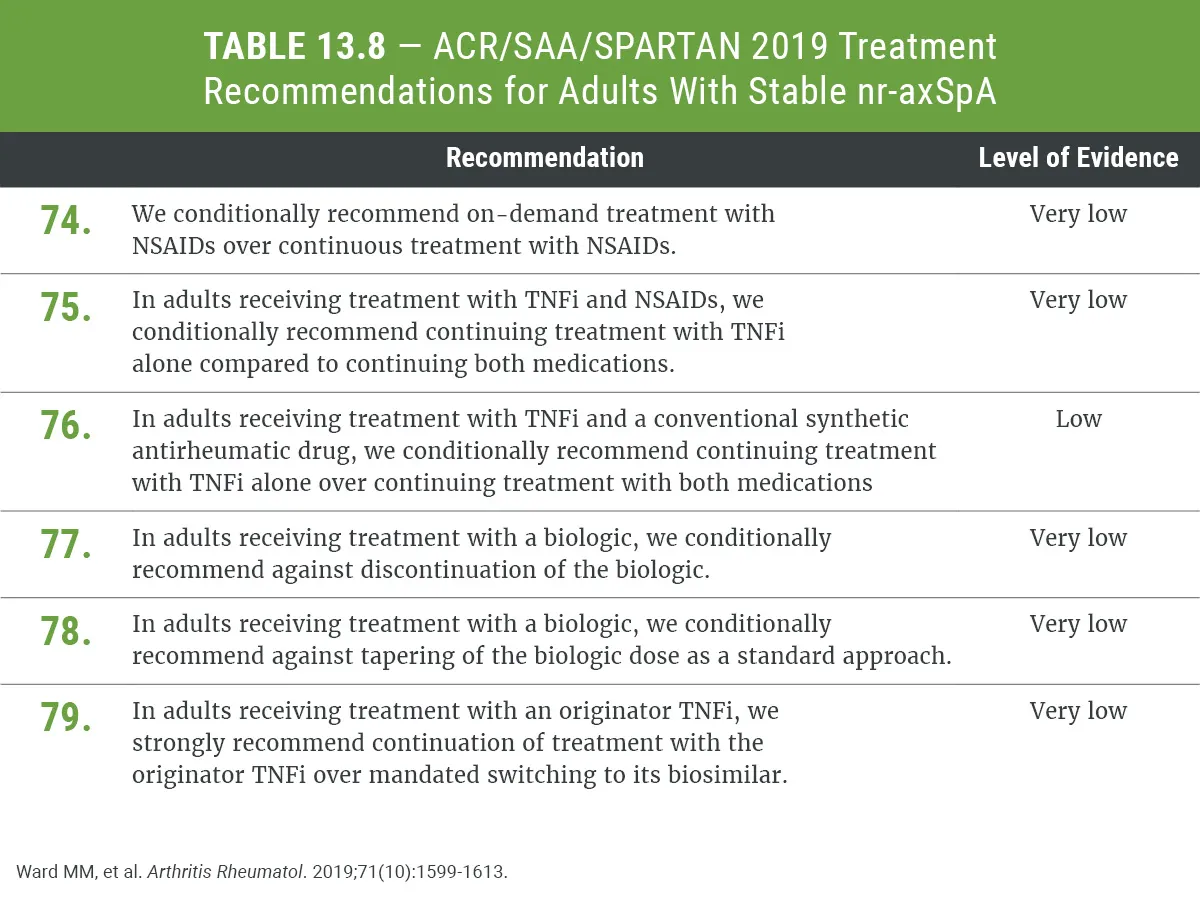
Medicine never stands still, and the ACR has already begun weaving newer therapies into its updates. In 2024, an addendum highlighted biosimilar switching as safe and costeffective. By 2025, JAK inhibitors entered the conversation for patients who cant tolerate TNF or IL17 blockers, although the guideline still lists them as conditional due to limited longterm safety data.
Are JAK inhibitors now part of the ACR recommendations?
Not as a firstline choice. The 2024 addendum notes theyre an option for refractory disease after failure or intolerance to both TNF and IL17 agents, provided the patient has no high cardiovascular risk.
What does the 2025 axial spondyloarthritis guideline say about biosimilars?
It treats biosimilars as interchangeable with their reference products, provided the patient is stable on the original medication. The recommendation is strong meaning you can confidently switch to a lowercost biosimilar without compromising efficacy.
Minitimeline of key updates (20192025)
| Year | Milestone |
|---|---|
| 2019 | Original ACR AS guideline released |
| 2022 | EULAR updates imaging recommendations |
| 2023 | ASASSPARTANSAA adds physiotherapy specifics |
| 2024 | ACR addendum endorses biosimilar switching |
| 2025 | New conditional language for JAK inhibitors |
Resources & Tools
To make the guidelines truly usable, the ACR provides downloadable PDFs, decisionaid apps, and patient handouts. Ive bookmarked a few favorites that you might find handy.
How to access the full ACR guideline free of charge?
Visit the ACRs official website and click the Guideline PDF button no login required. The file is under 5MB, so it loads quickly even on a phone.
Best patienteducation videos
Theres a concise 7minute animation on the Pathophysiology of AS hosted on the ACR YouTube channel; it uses clear visuals and plain language, making it perfect for sharing with a newly diagnosed friend.
Top5 downloadable resources
- Full ACR guideline PDF (official source)
- Shared decisionmaking worksheet (PDF)
- Physicaltherapy exercise booklet (PDF)
- Biologic safety monitoring checklist (PDF)
- Patientfriendly medication adherence calendar (PDF)
Conclusion
In a nutshell, the ACR ankylosing spondylitis guidelines give you a clear, evidencebased pathwayfrom pinpointing the diagnosis with the ASAS criteria to stepping through NSAIDs, physical therapy, and biologics while keeping safety front and center. They line up nicely with, yet have thoughtful differences from, the EULAR and ASAS recommendations, giving you flexibility to tailor care to your setting.
The real magic happens when you bring these recommendations into the exam room, explain the why behind each step, and involve patients in the decisionmaking process. Download the free resources, chat with your rheumatology team, and feel empowered to manage AS with confidence.
Got questions or personal experiences with the ACR guidelines? Drop a comment below Id love to hear how youre applying these recommendations in your practice or daily life. And if you found this guide helpful, share it with a friend who might need a friendly roadmap through the world of ankylosing spondylitis.
For related patient education on recovery after procedures, see this brief guide on post op recovery which can help clinicians advise patients who start biologics soon after surgery.
FAQs
What are the ACR ankylosing spondylitis guidelines?
The ACR (American College of Rheumatology) ankylosing spondylitis guidelines provide evidence-based recommendations for diagnosing and managing both radiographic and non-radiographic axial spondyloarthritis, covering pharmacologic treatments, imaging, and patient monitoring[1].
How does the ACR recommend diagnosing ankylosing spondylitis?
The ACR recommends using ASAS classification criteria, with additional emphasis on clinical suspicion, HLA-B27 testing, and targeted MRI use when X-rays are inconclusive, especially for non-radiographic disease[1].
What is the first-line treatment for ankylosing spondylitis according to ACR?
First-line treatment is NSAIDs (non-steroidal anti-inflammatory drugs) and supervised physical therapy; biologics (TNF inhibitors) are conditionally recommended if NSAIDs fail to control symptoms after 4 weeks[2].
When should biologics be considered in ankylosing spondylitis?
Biologics should be considered when disease activity remains high despite maximal NSAID therapy, or if MRI shows ongoing inflammation, especially in patients with persistently elevated CRP or BASDAI scores[2].
How do the ACR guidelines compare to EULAR for ankylosing spondylitis?
ACR guidelines emphasize clinical suspicion before ordering MRI, while EULAR suggests early MRI for all suspected cases. Both recommend TNF inhibitors as first-line biologics, but ACR also allows IL-17 inhibitors in select cases[1].