Below youll find everything you need to knowwhat an adrenal nodule actually is, why size matters, which symptoms (if any) you should watch for, what tests doctors usually order, and when treatment becomes necessary. Think of this as a friendly conversation with a knowledgeable buddy whos been through the same maze.
Adrenal Nodule Basics
What exactly is an adrenal nodule?
The adrenal glands are tiny, triangleshaped organs that sit on top of each kidney. Theyre like the bodys stressresponse factories, cranking out hormones such as cortisol, aldosterone, and adrenaline. A nodule is simply a small lump of tissue that shows up on imagingusually an incidental finding when youre being scanned for something unrelated (like a kidney stone or a back issue).
Benign vs. malignant how do doctors tell?
Most adrenal nodules turn out to be adenomas, which are harmless, noncancerous growths. A minority can be pheochromocytomas (hormoneproducing tumors) or, far more rarely, adrenal cortical carcinomas. Radiologists look at the nodules density, shape, and enhancement pattern on CT or MRI to guess its nature, but a definitive answer often requires hormonal testing or, in very select cases, a biopsy.
Realworld example
Take Jane, a 48yearold accountant. She went into the ER for sudden flank pain and, while getting a CT to rule out kidney stones, the radiologist spotted a 2cm nodule on her left adrenal gland. Jane felt a wave of anxietyShould I be worried about a nodule on my adrenal gland?but the doctor explained that most such nodules are benign. They ordered a simple blood test for hormone levels, and the results were normal. Janes followup plan? A repeat CT in nine months.
Size and Risk
Why does a 2cm measurement matter?
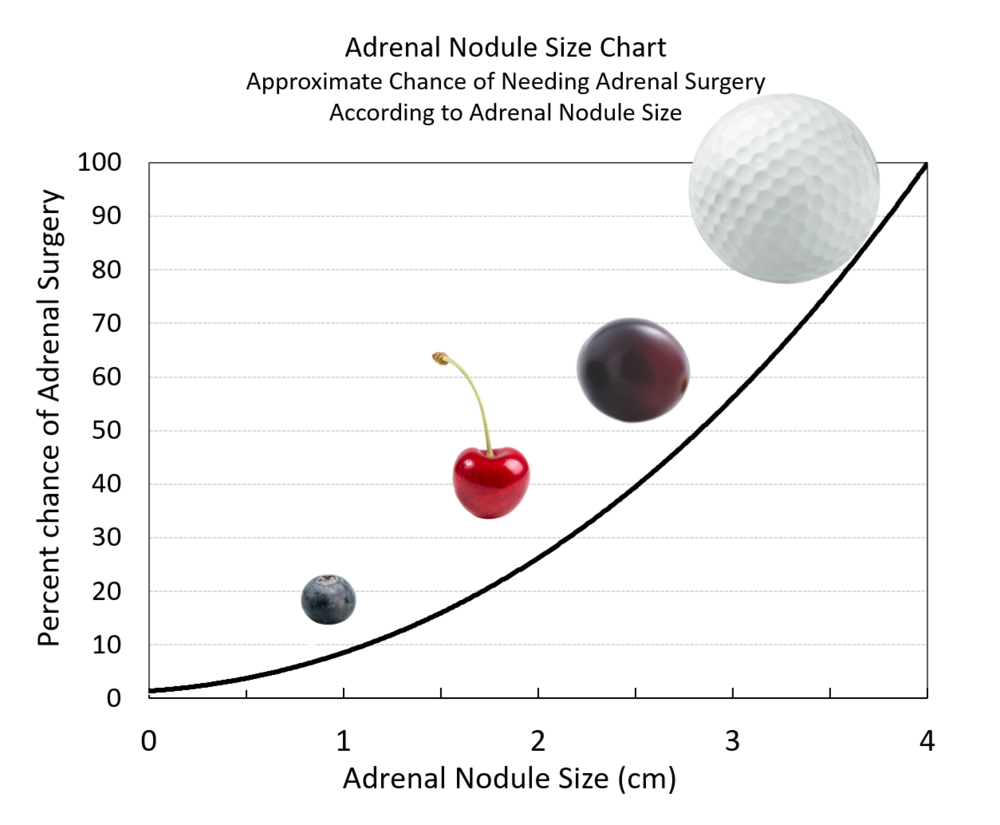
In adrenal imaging, size is a useful, though not decisive, risk factor. Nodules under 1cm are usually observed without any immediate followup. Those between 1cm and 4cmincluding our 2cm friendhave a high likelihood of being noncancerous, but they may still secrete hormones. Anything larger than 4cm raises red flags for malignancy and often triggers more aggressive workup.
Sizerisk correlation chart
| Size Range | Typical Risk | Usual Management |
|---|---|---|
| 1cm | Very low cancer risk; usually nonfunctioning | No immediate imaging; occasional repeat if symptoms develop |
| 12cm (including 2cm) | Lowtomoderate risk; hormoneproducing possible | Hormonal panel + repeat CT/MRI in 612months |
| 24cm | Higher chance of functional tumors; rare malignancy | Full hormonal workup; consider PETCT if suspicious |
| >4cm | Significant cancer risk | Surgical referral; comprehensive imaging and labs |
What about a 1cm or 2.5cm nodule?
A 1cm nodule on adrenal gland usually gets a watchful waiting approach; doctors might repeat imaging only if the patient develops symptoms. A 2.5cm adrenal nodule pushes you a little closer to the threshold where many endocrinologists start thinking about more detailed hormonal tests, especially if you have any blood pressure changes or unexplained weight fluctuations.
Symptoms to Watch
Nonfunctioning nodules are they silent?
Most incidental nodules dont produce hormones, meaning you wont feel any direct symptoms. In these cases, the nodule is essentially a quiet neighbor you happen to notice on a CT scan. Thats why many people with a 10mm left adrenal nodule never experience any issues at all.
Hormoneproducing nodules what can they cause?
If the nodule is actively secreting hormones, the body can send out a cascade of signals. Below are the classic symptom clusters:
- Aldosterone excess: Persistent high blood pressure, frequent headaches, muscle cramps, and occasional episodes of low potassium.
- Cortisol excess: Unexplained weight gain (especially around the midsection), thin skin that bruises easily, fatigue, and a moonshaped face.
- Catecholamine excess (pheochromocytoma): Sudden palpitations, sweating, paniclike anxiety attacks, and spikes in blood pressure that seem to come out of nowhere.
These are the benign adrenal gland tumor symptoms that many patients describe. If any of these sound familiar, let your doctor know right awayearly detection can make management much smoother.
Femalespecific concerns
Women sometimes notice hormonal imbalances differently, such as irregular menstrual cycles or unexplained hair growth. While an adrenal gland tumor symptoms in female can overlap with the general list, its worth mentioning to your healthcare provider because hormonedriven issues can affect fertility and overall quality of life.
Tests & FollowUp
Imaging options what will you see?
After the initial CT that discovered the nodule, doctors often order a contrastenhanced CT or an MRI to get a clearer view of the tissue characteristics. If theres suspicion of malignancy, a PETCT may be added to assess metabolic activity.
Hormonal workup the essential panel
Even if you feel fine, a prudent doctor will order a set of blood and urine tests to rule out hidden hormone production:
- Aldosterone/renin ratio screens for primary aldosteronism.
- Overnight dexamethasone suppression test checks for cortisol overproduction.
- Plasma metanephrines or 24hour urine catecholamines looks for pheochromocytoma.
According to the , a normal hormonal panel in a 2cm nodule typically leads to a watchful waiting schedule with repeat imaging in 612 months.
Followup schedule
Most endocrinology societies recommend a repeat CT or MRI at 6month intervals for the first year when a nodule is 12cm and the hormonal workup is negative. If the nodule remains stable in size and the labs stay normal, the interval can be extended to annually for a few years, then potentially discontinued after five years of stability.
Also consider checking related endocrine health topics that can affect metabolic balance; for example, readers concerned about hormone impacts on blood sugar may find it helpful to read about strawberries blood sugar as part of broader dietary considerations.
Practical tip keep a nodule tracker
Consider creating a simple spreadsheet with columns for date, imaging results, hormone levels, and any new symptoms. This Adrenal Nodule Tracker not only helps you stay organized but also makes your next doctors visit more efficient.
Treatment Options
Observation the power of patience
If the nodule is nonfunctioning and stable, the best treatment might be doing nothing at alljust keeping an eye on it. Regular scans and lab work are the only interventions, and many patients live symptomfree for years.
Medical management controlling hormone excess
When a nodule secretes aldosterone, doctors often start you on a mineralocorticoid receptor antagonist like spironolactone. For cortisol excess, medications such as ketoconazole or metyrapone can blunt hormone production while you decide on longerterm options. These drugs are usually welltolerated, but they do require periodic blood tests to monitor liver function and electrolytes.
Surgery when removal is the answer
Laparoscopic adrenalectomy is the standard approach for nodules that are clearly functional, rapidly growing, or larger than 4cm. The procedure has a high success rateup to 95% of patients experience resolution of hormonerelated symptomsand a relatively short recovery time (most are home within a week). According to the , postoperative complications are rare, especially when performed by an experienced endocrine surgeon.
Choosing the right path
Deciding between observation, medication, or surgery isnt a onesizefitsall calculation. It hinges on three pillars:
- Hormonal activity: Any excess hormone usually tips the scale toward treatment.
- Growth pattern: A nodule that enlarges by more than 0.5cm over a year often warrants removal.
- Patient preference: Some people prefer definitive surgery to avoid lifelong medication or imaging.
Bottom Line
Key takeaways
- Most 2cm nodules on adrenal glands are benign and asymptomatic.
- Hormoneproducing nodules can cause high blood pressure, weight changes, or anxietylike episodeswatch for those signs.
- A simple blood/urine panel plus a repeat scan in 612months is the standard safety net.
- Treatment ranges from watchful waiting to medication or laparoscopic surgery, depending on function, growth, and personal comfort.
When to call your doctor
If you notice any new hypertension, unexplained weight gain, palpitations, or changes in your menstrual cycle, reach out promptly. Even if you feel fine, a followup appointment within the next few weeks to discuss the hormonal panel results and imaging schedule will give you peace of mind.
Got more questions or personal experiences with adrenal nodules? Share them in the commentswere all in this together, and your story might help someone else navigate the same uncertainty.
Ready to take the next step? Download our free Adrenal Nodule Tracker PDF below, schedule your hormonal tests, and keep the conversation going with your healthcare team. Youve got this!
FAQs
What does a 2 cm nodule on the adrenal gland usually indicate?
Most 2 cm adrenal nodules are benign adenomas and cause no symptoms, but a small percentage can produce hormones or, rarely, be malignant.
How do doctors determine if the nodule is functioning?
A hormonal work‑up is ordered, including aldosterone/renin ratio, overnight dexamethasone suppression test, and plasma metanephrines or 24‑hour urine catecholamines.
What symptoms suggest the nodule might be hormone‑producing?
Signs can include high blood pressure, unexplained weight gain, muscle weakness, frequent headaches, palpitations, sweating, or menstrual irregularities.
When is surgical removal recommended?
Surgery is usually advised if the nodule is hormonally active, grows more than 0.5 cm per year, or exceeds 4 cm in size, indicating a higher cancer risk.
How often should follow‑up imaging be performed?
If the hormonal panel is normal, a repeat CT or MRI is recommended at 6–12 months; stable nodules can then be scanned annually for a few years.