Lets cut to the chase: the rareadenosquamous carcinoma (often shortened to ASC) is generally regarded as theworst type of colon cancer. It mixes the aggressive traits of squamous cells with the spreadpotential of adenocarcinoma, which means it tends to grow fast, spread early, and shrug off many standard treatments.
If youre wondering how to tell whether a tumor falls into this worst category, look for three telltale signs speed of growth, likelihood of early metastasis, and resistance to typical chemoregimens. Below well walk through what makes a colon cancer type the worst, which rare cancers you should keep on your radar, and what steps you can take if you suspect something serious.
Defining the Worst
What makes a type worst?
Theres no official medical label called worst type, but doctors use a handful of criteria to judge how dangerous a tumor is. Think of it as a grading system that looks at how quickly the cells divide, how far theyve traveled by the time theyre found, and whether they respond to the drugs we have on hand.
Oncologists criteria
When a specialist evaluates a colon cancer, they generally consider:
- Grade: Poorly differentiated cells (they look very messy under a microscope) usually signal a highergrade, more aggressive cancer.
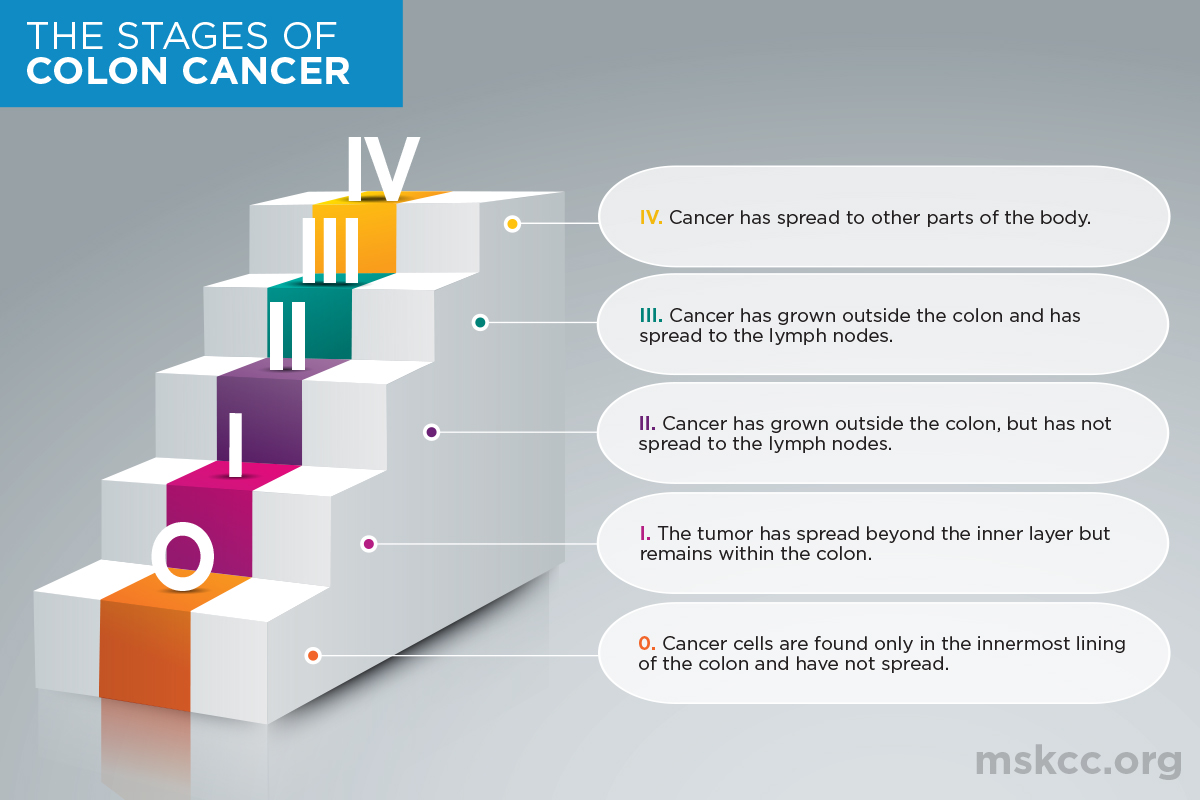
- Stage at diagnosis: Cancers caught at stageIII or IV have already spread to lymph nodes or distant organs.
- Molecular profile: Mutations in KRAS, NRAS, or a lack of microsatellite instability (MSIH) can make a tumor tougher to treat.
Comparison of Types
| Cancer Type | Typical Aggressiveness | 5Year Survival |
|---|---|---|
| Adenocarcinoma (common) | Moderate | 65% |
| SignetRing Cell | High | 30% |
| Adenosquamous Carcinoma (ASC) | Very High | 12% |
| Mucinous Adenocarcinoma | High | 45% |
These numbers come from recent survival statistics and give a quick snapshot of why ASC tops the worst list.
Rare Aggressive Cancers
Adenosquamous carcinoma
ASC accounts for less than1% of all colorectal cancers. Its twin personalityboth glandular (adenocarcinoma) and squamouslets it break through tissue barriers faster than most tumors. Median survival hovers around 12months even with aggressive therapy, which is why its flagged as the worst.
Signetring cell cancer
This variety gets its name from the way the cancer cells look under a microscope: they have a big vacuole pushing the nucleus to the side, resembling a signet ring. It tends to spread to the peritoneum (the lining of the abdomen) early, making surgery less effective.
Mucinous adenocarcinoma
When a tumor produces an excess of mucus (over60% of its volume), its called mucinous. The slime helps cancer cells slip through the colon wall, leading to quicker spread, especially on the right side of the colon.
Neuroendocrine largecell carcinoma
Though rare, largecell neuroendocrine cancers grow like a wildfire. They often secrete hormones that cause odd symptomslike flushing or uncontrolled sweatingmaking them tricky to spot early.
Fact Sheet
- Prevalence: <1% for ASC, 12% for signetring, 510% for mucinous.
- Typical age at diagnosis: 5070years, but aggressive types can appear earlier.
- Key molecular markers: CK5/6 and p40 (squamous), MUC2/MUC5AC (mucinous), ChromograninA (neuroendocrine).
- Common locations: ASCany colon segment; Signetringright colon; Mucinousright colon.
Warning Symptoms
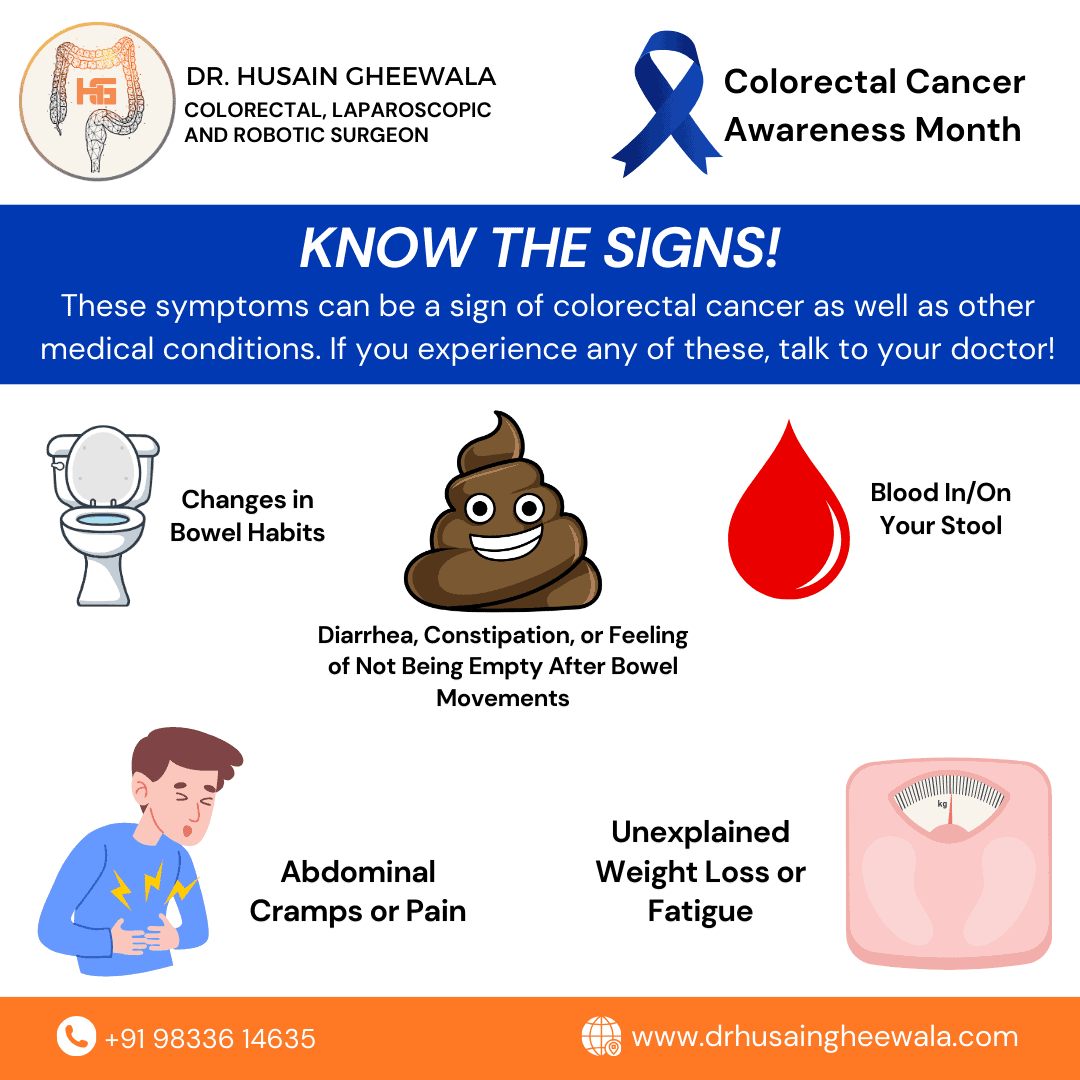
Common redflag signs
Most colon cancersaggressive or notshow up with a handful of classic warnings:
- Persistent abdominal pain or cramping.
- Changes in bowel habits lasting more than two weeks (constipation or diarrhea).
- Blood in the stool, which may appear bright red or as dark, tarry coffeeground material.
- Unexplained irondeficiency anemia.
Symptoms of rare types
Rare, aggressive forms tend to add a few extra clues:
- Rapid, unintentional weight loss.
- Feeling unusually full or bloated (ascites) even after a small meal.
- Persistent nausea or vomiting, especially with signetring cell spread to the peritoneum.
- Sometimes, a sensation of something stuck in the rectum that doesnt go away.
Symptom Checklist
| Check if you have: | What it might mean |
|---|---|
| Blood in stool | Possible bleeding from any colon tumor |
| Unexplained weight loss | Red flag for aggressive or advanced disease |
| Persistent abdominal pain | Could signal tumor growth or obstruction |
| Sudden change in bowel habits | Early sign of colon cancer |
| Bloating/ascites | Often seen with mucinous or signetring cancers |
Notice anything? If a symptom sticks around longer than two weeks, its wise to give your doctor a call.
Diagnosis Process
Colonoscopy and biopsy
The goldstandard test is a colonoscopy. A specialist slides a flexible camera through your colon, looks for suspicious lesions, and snags a tiny tissue sample. That sample becomes the basis for everything that follows.
Pathology and markers
In the lab, a pathologist stains the sample to see which cells are present. For ASC, theyll look for both adenocarcinoma markers (like CK20) and squamous markers (CK5/6, p40). Mucinous cancers light up with mucin stains (MUC2, MUC5AC), while neuroendocrine types shout out ChromograninA and Synaptophysin.
Imaging for staging
Once the tumors nature is confirmed, imaging steps in to map its spread:
- CT scan: Gives a quick overview of the abdomen and chest.
- MRI: Offers higher detail of soft tissues, especially useful for rectal involvement.
- PETCT: Highlights metabolically active disease, catching metastases that other scans miss.
Molecular testing
Modern oncologists also run genetic panels looking for KRAS, NRAS, BRAF mutations and microsatellite instability (MSI). These results guide whether you might benefit from targeted drugs or immunotherapy.
Sample pathology report
| Section | Findings |
|---|---|
| Histology | Adenosquamous carcinoma mixed glandular and squamous differentiation. |
| Immunohistochemistry | Positive CK5/6, p40; CK20 positive; MUC2 negative. |
| Stage | T3 N2 M1 (colon wall invasion, 4+ lymph nodes, distant metastasis). |
| Molecular | KRAS wildtype, MSIstable. |
Treatment Options
Surgery basics
When the tumor is still resectable, surgeons aim for an enbloc removaltaking out the affected segment of colon along with surrounding tissue and nearby lymph nodes. Clear margins (no cancer cells at the cut edge) are crucial; otherwise, the disease often returns.
Chemotherapy regimens
Standard firstline chemo usually involves FOLFOX (5FU, leucovorin, oxaliplatin) or FOLFIRI (5FU, leucovorin, irinotecan). For aggressive types like ASC, adding a biologic agent such as bevacizumab (an antiVEGF drug) is common, though response rates remain modest.
Targeted & immunotherapy
If the tumor shows high microsatellite instability (MSIH), checkpoint inhibitors like pembrolizumab can work wonders. Unfortunately, most worst tumors are microsatellite stable (MSS), limiting the effectiveness of immunotherapy. Ongoing research is exploring new combinationsread about it in a recent review.
Clinical trials
Because rare aggressive cancers have few proven treatments, enrolling in a clinical trial is often the best shot at cuttingedge therapy. Check for studies that accept patients with ASC or other rare histologies.
Decisionmaking flowchart
- Diagnosis Determine cancer type & stage.
- Is the tumor resectable?
Yes Surgery Adjuvant chemo biologic. - No Neoadjuvant chemo Reassess for surgery.
- Is MSIH present?
Yes Consider immunotherapy.
No Standard chemo + possible trial. - Throughout Supportive care (nutrition, counseling).
Real Patient Stories
How I knew I had colon cancer
I remember the day I first noticed blood in my stool. I brushed it off as hemorrhoidsyeah, I know, classic mistake. A few weeks later, I was feeling unusually fatigued, despite eating ironrich foods. My doctor ordered a colonoscopy, and the biopsy came back as signetring cell carcinoma. It was a shock, but early detection saved my life.
A surprise ASC diagnosis
My friend Jess thought she had a routine gastroupset. Shed been battling chronic constipation for months, then started gaining weight around her bellya weird, bloated feeling. When doctors finally performed a CT scan, they found a thickened segment of her colon. The pathology report shouted adenosquamous carcinoma. Jess was terrified, but joining a trial that combined chemo with a new targeted agent gave her hope. Today, shes in remission and loves sharing her story to warn others.
Conclusion
In the world of colorectal cancer, the adenosquamous carcinoma stands out as the worst type of colon cancer due to its rapid growth, early spread, and limited response to traditional therapies. Yet understanding the redflag symptoms, getting prompt, thorough diagnostics, and exploring all treatment avenuesincluding clinical trialscan make a lifesaving difference. If anything in this article resonated with you, or you have questions about your own health, dont hesitate to reach out to a trusted gastroenterologist or oncologist. Knowledge is power, and together we can face even the toughest diagnoses with confidence.
For readers concerned about cancer-related skin changes or discoloration that sometimes accompany advanced disease or treatment, resources on cancer skin discoloration may be helpful and provide practical guidance.