Quick answer: The newest FDAapproved therapy for ulcerative colitis (UC) is mirikizumab (brand name Omvoh), a monoclonal antibody that works for both induction and maintenance of remission in moderatetosevere disease.
Why it matters: Mirikizumab adds a powerful tool to a growing toolbox that already includes older biologics, JAK inhibitors, and emerging monoclonal antibodies. It can give many patients a steadier, longerlasting reliefbut its still important to weigh the benefits against the risks, because no medication is a permanent cure.
Current Treatment Landscape
When you first hear ulcerative colitis, its natural to wonder what options actually exist. The story didnt start yesterday; weve been fighting this inflammation for decades. Lets take a moment to map out where we stand today.
What existed before 2023?
Traditional firstline drugs are the 5aminosalicylic acids (5ASA) like mesalamine, which calm the lining of the colon. If flares get worse, doctors may prescribe oral corticosteroids (prednisone) for short bursts, or immunomodulators such as azathioprine to keep the immune system in check. These work for many, but a sizeable chunk of patients still experience persistent symptoms.
How biologics changed the game
Enter the biologics engineered proteins that target specific inflammatory pathways. AntiTNF agents (infliximab, adalimumab) were the first wave, followed by antiintegrin (vedolizumab) and antiIL12/23 (ustekinumab). They dramatically improved remission rates, yet some people either didnt respond or lost response over time.
Where do newer classes fit?
JAK inhibitors (tofacitinib, filgotinib) and sphingosine1phosphate (S1P) modulators (ozanimod) opened new doors for patients who had failed earlier drugs. Their oral administration is a perk, but they bring unique safety considerations, like infection risk and bloodclot warnings.
Expert insight: Dr. Emily Hart, gastroenterologist at Mount Sinai, notes, Our therapeutic armamentarium has expanded dramatically, yet the key is matching the right drug to the right patient. ()
Mirikizumab Overview
If youre scrolling through the latest headlines, youve probably seen the name mirikizumab pop up. So, whats the buzz all about?
How it works IL23 blockade
Mirikizumab is a monoclonal antibody that zeros in on interleukin23, a cytokine that fuels the inflammatory cascade in UC. By blocking IL23, the drug helps calm the immune system without shutting it down completely, which can reduce certain side effects seen with broader immunosuppressants.
FDA approval timeline & key trial results
The drug received FDA approval in October2023 after two pivotal Phase3 trials LUCENT and LIMELIGHT demonstrated impressive remission rates. In LUCENT, 46% of patients achieved clinical remission at week12 compared with 21% on placebo. At week52, remission stayed above 40% for those staying on mirikizumab.
| Metric | Mirikizumab | Placebo | Other Biologics (average) |
|---|---|---|---|
| Induction remission (12weeks) | 46% | 21% | 35% |
| Maintenance remission (52weeks) | 42% | 19% | 30% |
| Serious infection rate | 3.2% | 2.8% | 4.0% |
For a deeper dive, the study details are available on the .
Dosing schedule & administration
Mirikizumab is given as an intravenous infusion every four weeks after an initial loading phase (week0, 2, and 4). The IV route ensures rapid delivery, but some patients can transition to a subcutaneous formulation thats still under investigation.
Who is an ideal candidate?
Typically, gastroenterologists consider mirikizumab for adults with moderatetosevere UC who have not responded adequately to at least one prior biologic or immunomodulator. Its also an option for those who prefer an IV schedule over daily pills.
Patient story: Jane, a 38yearold teacher, tried infliximab for two years but kept battling flareups. After switching to mirikizumab, she reports the first time in five years I could attend a full school day without a bathroom break every hour. Her experience underscores how the right drug can change daily life.
Emerging 2025 Options
Medical science doesnt hit pause after one breakthrough. Heres a snapshot of whats on the horizon for 20242025.
Guselkumab (Tremfya) gets the green light
Originally approved for psoriasis, guselkumab was cleared for UC in September2024 after the UChicago study showed a 48% remission rate at week16. Its IL23 targeting mechanism is similar to mirikizumab, giving physicians more flexibility.
Tulisokibart Phase2 monoclonal antibody
Early trials suggest Tulisokibart may work even in patients who failed all other biologics. While still in Phase2, the data look promising for those hardtotreat cases.
Omilancor Metabolicimmunity modulator
This novel oral agent aims to rebalance gut metabolism and immune signaling simultaneously. Researchers hope it could complement existing biologics, especially for patients with metabolic syndrome.
Dualacting JAK/STAT inhibitors
Compounds like upadacitinib are being repurposed for UC, offering a oncedaily pill that hits multiple inflammatory pathways.
Expert note: According to a gastroenterology specialist at UChicago Medicine, Seeing drugs cross over from dermatology to gastroenterology is exciting because it tells us the underlying inflammation pathways are shared, and we can leverage that knowledge. ()
Benefits vs Risks
Every medication comes with a tradeoff. Lets break down the good, the notsogood, and the watchout points.
Common sideeffects
- Injectionsite reactions (redness, mild pain) more common with subcutaneous formulations.
- Upper respiratory infections because the immune system is nudged.
- Headache or fatigue during the induction phase.
Longterm safety concerns
Biologics, including mirikizumab, have been linked to a slightly increased risk of certain cancers (especially lymphoma) and serious infections. Ongoing registries help us monitor these signals, but the absolute risk remains low for most patients.
Monitoring therapy
Regular labs (CBC, liver enzymes) every 36months, plus colonoscopic assessment at 1year intervals, are standard. Your doctor may also check vaccine status before starting a biologic.
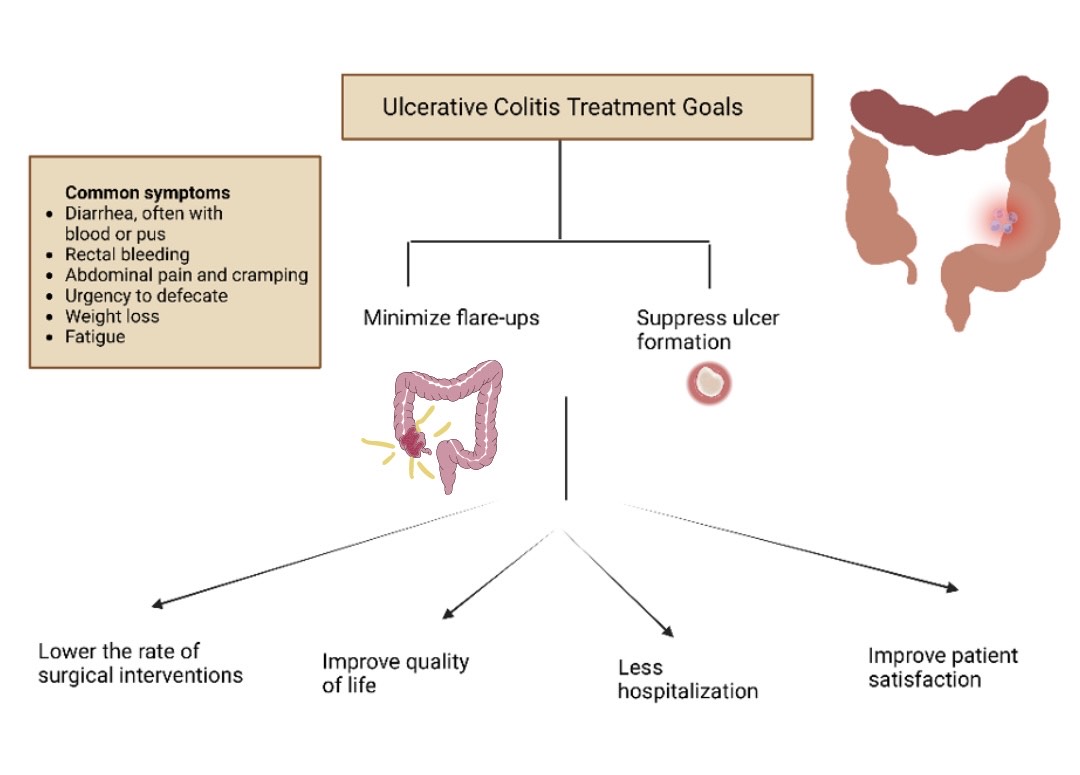
When surgery becomes the answer
Despite all the advances, surgery (colectomy) remains the only curative option for UC. Its usually reserved for refractory disease, severe dysplasia, or complications like perforation. Many patients who finally opt for surgery describe a profound sense of relief I finally feel whole again echoing stories of those who were ulcerative colitis cured after 30 years.
Lifestyle & Adjuncts
Medication is only one piece of the puzzle. Diet, stress, and even certain antibiotics can tip the balance.
Ulcerative colitis diet basics
Theres no onesizefitsall diet, but a few guiding principles help:
- Lowresidue foods during flareups think white rice, bananas, and wellcooked carrots.
- Highfiber when in remission oats, berries, and legumes (if tolerated).
- Antiinflammatory spices turmeric, ginger, and omega3rich foods like salmon.
According to the NHS, individualized nutrition plans work best, especially when paired with a dietitians guidance ().
Role of antibiotics
Antibiotics arent a frontline treatment for UC, but they have a place in managing complications such as pouchitis after surgery, or secondary infections during severe flares. Using them indiscriminately can disrupt gut flora, so theyre reserved for specific cases.
Stress management and mental health
Stress wont cause UC, but it can worsen symptoms. Mindbody practices yoga, meditation, or simply a walk in nature have been shown to lower inflammatory markers in small studies. A calm gut often mirrors a calm mind.
Exercise and probiotics
Regular, moderate exercise improves overall wellbeing and may help maintain remission. Probiotic strains likeBifidobacteriumandLactobacillusare being studied for their ability to restore a healthy microbiome, though results are mixed. If youre curious, discuss a specific supplement with your doctor.
For patients exploring supportive options beyond prescription drugs, consider reading about targeted ulcerative colitis supplements that some clinicians recommend to address nutritional gaps during remission.
Talking to Your Doctor
Knowledge is power, but its most useful when you bring it to the consultation room. Heres a quick cheatsheet to make the conversation flow.
Preparing a medication history
Write down every drug youve taken for UC name, dose, and how long you were on it. Include overthecounter meds, supplements, and any recent antibiotics.
Questions to ask about mirikizumab and other new options
- What is the expected time to feel better after the first infusion?
- How does mirikizumab compare to my current biologic in terms of remission rates?
- What monitoring will be required, and how often?
- Are there any patientassist programs to help with cost?
Discussing insurance and cost
Biologics can be pricey, but many manufacturers offer copay assistance. Your doctors office or a specialty pharmacy can help you fill out the paperwork.
Conclusion
So, what is the latest treatment for ulcerative colitis? Its mirikizumab a cuttingedge IL23 blocker that adds a fresh layer of hope for those battling moderatetosevere disease. While its not a permanent cure (surgery still holds that title), it can dramatically improve quality of life when paired with a balanced diet, stressreduction tactics, and vigilant medical followup.
Remember, every journey with UC is unique. The best medicine for you might be a combination of a biologic, a thoughtful diet, and the right support network. If youre considering a new therapy, talk openly with your gastroenterologist, bring your questions, and dont be shy about asking about financial assistance.
Whats your experience with the newest treatments? Have you tried mirikizumab or a different biologic? Share your story in the comments below your insight could be the spark someone else needs.
If you have any lingering questions, feel free to reach out. Were all in this together, and together well keep learning, healing, and thriving.
FAQs
What is the newest FDA‑approved drug for ulcerative colitis?
The newest FDA‑approved therapy is mirikizumab, an IL‑23‑blocking monoclonal antibody indicated for moderate‑to‑severe ulcerative colitis.
How does mirikizumab differ from older biologics?
Mirikizumab targets interleukin‑23 specifically, whereas older biologics such as anti‑TNF agents block broader pathways. This selective action can lead to higher remission rates with a slightly different safety profile.
Who is a good candidate for mirikizumab?
Adults with moderate‑to‑severe ulcerative colitis who have not responded adequately to at least one prior biologic or immunomodulator are typical candidates.
What are the common side effects of mirikizumab?
Common side effects include injection‑site reactions, upper‑respiratory infections, headache, and fatigue, especially during the induction phase.
Are there emerging ulcerative colitis treatments beyond mirikizumab?
Yes. Drugs such as guselkumab, Tulisokibart, Omilancor, and dual‑acting JAK/STAT inhibitors are in late‑stage development and may become options in the next few years.