If a sudden, chaotic heartbeat hits you or a loved one, the first thing doctors do is a quick electrical shock thats the fastest, lifesaving VFib treatment. In the next few minutes youll learn exactly what that shock looks like, which medicines back it up, and what longterm steps keep the rhythm steady.
Well walk through the whole journey: from the emergency defibrillation, through the meds you might see in the ER, to the devices and lifestyle tweaks that help people live full lives after a VFib scare. Ready? Lets dive in together.
Why VFib Matters
What is ventricular fibrillation?
Ventricular fibrillation (VFib) is a rapid, erratic electrical storm in the hearts lower chambers. Instead of a coordinated beat, the ventricles quiver like a shaken soda can, producing no useful pumping action. On an ECG youll spot a wildly wiggly line with no discernible QRS complexes the classic vfib ecg pattern.
Typical VFib symptoms
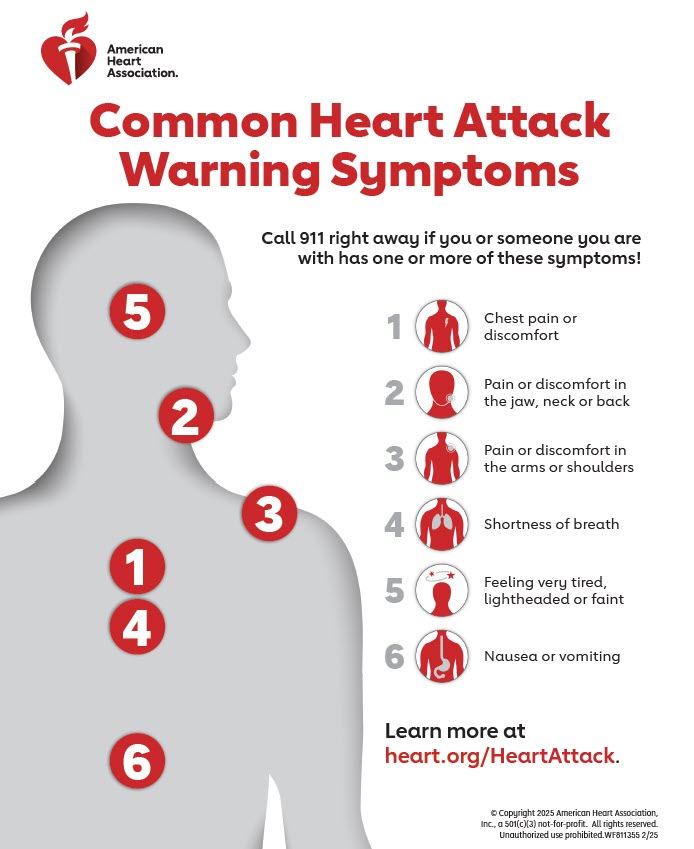
Most people dont feel a gradual symptom buildup. VFib usually shows up as sudden collapse, loss of pulse, or no breathing after a brief bout of chest discomfort. Bystanders might hear a thudding heart or feel no pulse at all. Because the heart stops delivering blood, every second counts.
Realworld snapshot
Imagine Sarah, a 42yearold runner, feeling a sudden whoosh in her chest during a jog. She collapses, and a friend immediately starts CPR while calling 911. Within two minutes, a defibrillator delivers a shock and her heart clicks back into rhythm. Stories like Sarahs illustrate why rapid action is the cornerstone of vfib treatment acls protocols.
FirstLine Treatment
Defibrillation GoldStandard Shock
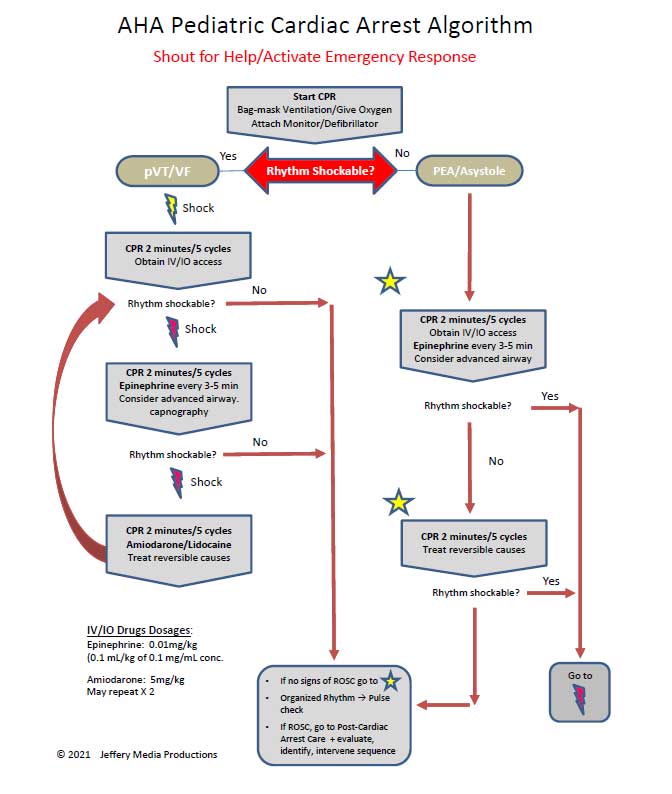
The moment a VFib rhythm is confirmed, an automated external defibrillator (AED) or manual defibrillator delivers a controlled electric shock. The goal? Reset the hearts electrical system so the natural pacemaker can regain control.
According to the , the recommended energy dose for a first shock is 200 joules (biphasic). If the rhythm persists, subsequent shocks follow the vfib algorithm in the ACLS guidelines.
QuickReference Defibrillation Table
| Step | Action | Details |
|---|---|---|
| 1 | Assess rhythm | VFib confirmed on monitor |
| 2 | Charge defibrillator | 200J biphasic (first shock) |
| 3 | Pause compressions | 5seconds, then deliver shock |
| 4 | Resume CPR | 30 compressions, 2 breaths |
| 5 | Reassess | Check rhythm; repeat up to 3 shocks |
Highquality CPR while waiting
Defibrillation isnt the only hero. While the shock is prepared, highquality chest compressions keep blood flowing. Aim for a depth of at least 2inches, a rate of 100120 per minute, and full chest recoil. A compressiontoventilation ratio of 30:2 is standard for adults.
Medication after the third shock
If after three shocks the rhythm stubbornly stays chaotic, meds enter the scene. The two main drugs are:
- Epinephrine 1mg IV/IO every 35minutes to boost coronary perfusion.
- Amiodarone 300mg IV bolus, followed by 150mg if needed, for antiarrhythmic control.
Lidocaine is an alternative when amiodarone isnt available. A 2024 notes that early epinephrine improves shortterm ROSC (return of spontaneous circulation), while amiodarone helps maintain a stable rhythm longer term.
Continued Care Options
Implantable CardioverterDefibrillator (ICD)
For anyone whos survived a VFib episode, an ICD is often the next line of defense. It continuously monitors heart rhythm and delivers a shock automatically if VFib reappears. Think of it as a personal bodyguard thats always on standby. Patients with underlying DI heart failure may particularly benefit from ICD placement for preventing fatal arrhythmias.
Catheter Ablation & Advanced Procedures
When the VFib source is a scarred area from a prior heart attack, a catheter can be steered to the problematic tissue and ablate (burn) it, reducing future episodes. More rarely, cardiac sympathetic denervation a surgery that cuts nerves feeding the hearts electrical system may be considered for refractory cases. The reports success rates of up to 70% in select patients.
Medication for secondary prevention
Beyond the emergency, doctors often prescribe:
- Betablockers lower heart stress and reduce arrhythmia triggers.
- Antiarrhythmics such as amiodarone (maintenance dose) or ranolazine for certain electrical abnormalities.
These drugs help keep the hearts electrical environment stable, especially when combined with lifestyle adjustments.
ICD vs. Ablation vs. Meds Comparison
| Option | Pros | Cons | Typical Candidate |
|---|---|---|---|
| ICD | Automatic shock, proven survival benefit | Device infection, battery replacements | Anyone postVFib or highrisk structural heart disease |
| Ablation | Potentially reduces need for shocks | Invasive, not always successful | Scarrelated VFib, drugrefractory cases |
| Meds | Noninvasive, easy to adjust | Sideeffects, adherence needed | Patients unsuitable for procedures or as adjunct therapy |
Living With VFib
Survival odds with immediate treatment
When defibrillation occurs within the first few minutes, survival can exceed 90%. A study found that each minute of delay reduces survival by about 710%.
Prognosis without treatment
Without a prompt shock, VFib is almost always fatal within minutes due to brain hypoxia. Thats why every second counts and why public AEDs are lifesavers in schools, airports, and workplaces.
Patient story five years later
Mike, a 58yearold accountant, suffered a cardiac arrest at home. The EMTs shocked him, and an ICD was implanted two weeks later. Five years on, hes back on the golf course, with only occasional device checkups. His experience shows that life after VFib isnt just possible it can be thriving.
Risks & Benefits
Benefits of each treatment tier
- Defibrillation Immediate restoration of circulation, can be the difference between life and death.
- Medications Stabilize the heart, reduce recurrence, and are easily adjusted.
- ICD Provides continuous protection, often eliminating the need for emergency interventions.
Potential complications
Every intervention carries tradeoffs. Defibrillation can cause minor skin burns, although rare. ICDs may lead to infection or inappropriate shocks (the device shocking when its not needed). Antiarrhythmic meds can cause thyroid issues (amiodarone) or lung toxicity. Discussing these risks with a cardiologist ensures you weigh them against the lifesaving benefits.
Decisionmaking checklist
- Do I have a clear source of VFib (e.g., scar tissue)?
- Am I a candidate for an ICD based on age and overall health?
- What are my lifestyle goals (exercise, travel, work) and how might each option affect them?
- Do I understand the medication schedule and potential side effects?
Getting the Right Care
Key questions for your cardiologist
When you schedule that followup, bring these questions:
- Do I need an ICD, or can we try medication first?
- What lifestyle changes lower my risk of another VFib episode?
- How often should I have device checks or ECG monitoring?
- Are there clinical trials or newer therapies I should know about?
Resource list
For deeper dives, consider these reputable sources:
Conclusion
When ventricular fibrillation strikes, the fastest, most effective response is an immediate shock, followed by highquality CPR and targeted medications. After the crisis, longterm safeguardsICDs, catheter ablation, or wellchosen drugshelp people not just survive but thrive. Understanding the benefits and possible downsides of each step lets you, your family, and your healthcare team make informed, confident choices.
Have you or someone you love experienced VFib? Share your story or drop a question below; together we can turn a frightening moment into knowledge that saves lives.
FAQs
What is the first action to take when someone collapses from VFib?
Call 911 immediately, start high‑quality chest compressions, and retrieve an AED (automated external defibrillator) as soon as possible.
How does an AED help in VFib treatment?
An AED analyzes the heart rhythm and, if VFib is detected, delivers a controlled electric shock that can reset the heart’s electrical activity and restore a normal rhythm.
When is an implantable cardioverter‑defibrillator (ICD) recommended?
An ICD is typically advised for patients who have survived a VFib episode or have a high risk of recurrence due to underlying heart disease, scar tissue, or genetic arrhythmia syndromes.
Which medications are used during emergency VFib management?
Epinephrine (1 mg IV/IO every 3‑5 minutes) is given to improve coronary perfusion, and amiodarone (300 mg IV bolus, then 150 mg) is used to help maintain a stable rhythm if shocks alone are ineffective.
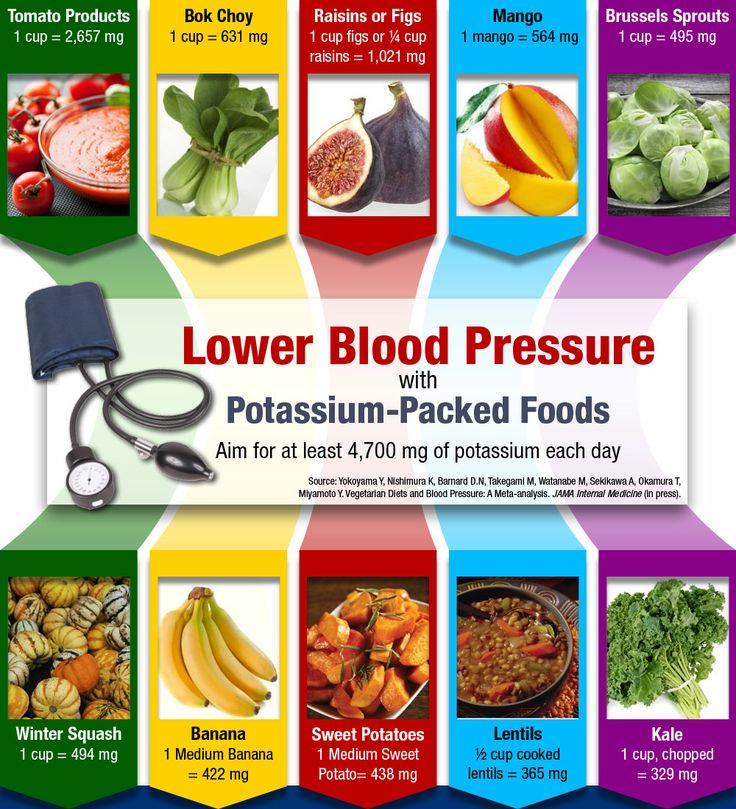
Can lifestyle changes lower the risk of VFib returning?
Yes. Maintaining a heart‑healthy diet, regular moderate exercise, controlling blood pressure and cholesterol, avoiding smoking, and adhering to prescribed medications all reduce the likelihood of another VFib episode.