Thinking about surgery for ulcerative colitis can feel like standing at a crossroads, and you deserve a clear, honest answer right away. In a nutshell, surgeryusually a proctocolectomy with a J-pouchremoves the diseased colon and offers a chance at lasting remission. Below you'll find the success rates, recovery timeline, costs, risks, and what life looks like after the operation, all laid out in a friendly, no-fluff style.
Why Surgery Matters
When is surgery recommended?
Most folks start with medicines, but when they stop working, flare-ups become severe, or there's a risk of dysplasia or cancer, doctors suggest surgery. It's not a first-line choice; it's a step taken when quality of life starts to slip. For some patients considering long-term management, optimizing medical therapy and supplements can be useful before deciding on surgerydiscuss options like ulcerative colitis supplements with your gastroenterology team as part of that conversation.
Types of ulcerative colitis surgery
The big players are:
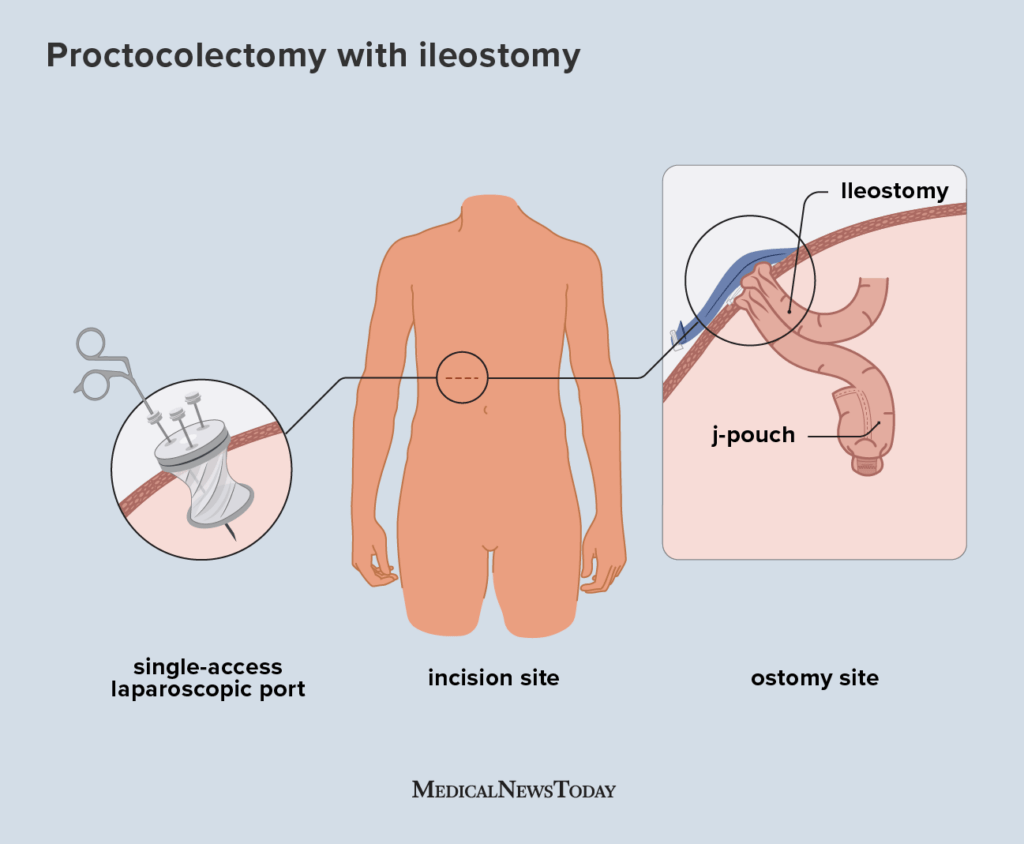
- Proctocolectomy with ileal pouch-anal anastomosis (J-pouch) the most common, aims to keep bowel continuity.
- Total colectomy with permanent ileostomy an external bag collects waste.
- Subtotal colectomy or surgery without a pouch leaves part of the rectum intact, often for specific medical reasons.
Quick comparison
| Procedure | Typical Indication | Pros | Cons |
|---|---|---|---|
| J-pouch | Failed meds, dysplasia | No permanent bag; near-normal continence | Risk of pouchitis; longer recovery |
| Permanent ileostomy | Severe disease, poor pelvic floor | Simpler surgery; predictable outcomes | External appliance; lifestyle adjustment |
| Without pouch | Specific anatomical concerns | Avoids pouch complications | May need future surgery; possible rectal disease |
Success Rate & Outcomes
Overall success statistics
Modern data show a 9095% long-term remission rate after a well-performed J-pouch. A cohort study of over 3,000 patients confirmed these numbers, with most enjoying a symptom-free life.
Factors that influence success
Surgeon experience mattersa high-volume colorectal surgeon (50 ulcerative colitis resections annually) dramatically lowers leak rates. Minimally invasive techniques (laparoscopic or robotic) also speed healing and reduce scar tissue. Younger patients and those without severe preoperative inflammation tend to have smoother recoveries.
Risks & Complications
Common short-term risks
Every operation carries a baseline risk: bleeding, infection, and anastomotic leaks are the usual suspects. Most surgeons mitigate these with prophylactic antibiotics and careful intraoperative testing.
Long-term complications
About 1530% of J-pouch patients develop pouchitis inflammation of the new pouch. While treatable with antibiotics, a minority may need repeat surgery. Other possible issues include pelvic sepsis, adhesions, and, in rare cases, pouch failure requiring a permanent ileostomy.
How to mitigate risks
Preoperative optimization (nutritional support, smoking cessation, and managing anemia) sets the stage for success. Choosing a surgeon who uses minimally invasive approaches and follows a strict post-op monitoring protocol can catch complications early.
Real-world example
Jenny, a 34-year-old graphic designer, shared that early detection of pouchitis during her 6-week follow-up saved her from a severe flare-up. She now tracks her stool pattern daily and contacts her gastroenterology team at the first sign of change.
Recovery & Life
Typical hospital stay and immediate recovery
For laparoscopic J-pouch procedures, most patients leave the hospital after 4872hours. You'll spend the first few days managing pain with IV meds, learning how to empty the new pouch, and getting up for short walks.
Return to work and normal activities
Most people feel ready to return to light duties within 46 weeks, and to full work by 8 weeks. Heavy lifting and intense exercise should be avoided until your surgeon gives the green lightusually around the 12-week mark.
Nutrition and bowel habits post-J-pouch
Diet starts with clear liquids, progresses to soft foods, and finally a normal diet over 23 weeks. Hydration is keyaim for at least 2 liters a dayto keep stool soft. Introducing soluble fiber slowly can help regulate frequency without causing blockages.
Day-by-Day checklist
| Time Frame | What to Expect |
|---|---|
| Day 13 | IV pain control, gentle ambulation, begin clear liquids. |
| Week 2 | Transition to soft foods, start pelvic floor exercises. |
| Month 1 | Regular bowel routine, monitor for pouchitis symptoms. |
| Month 3 | Full diet, return to work (if applicable), continue follow-up. |
Living without a pouch (permanent ileostomy)
If a J-pouch isn't suitable, a permanent ileostomy can be the safest route. It involves an external bag that collects waste. Modern appliances are discreet, waterproof, and many patients report a quick return to daily activitiesoften within two weeks.
Patient-experience snippet
Mike, a 58-year-old teacher, says, "I was nervous about the bag, but the newer pouch system feels like a small accessory. I'm back in the classroom faster than I imagined."
Cost Considerations
What does the procedure cost?
In the United States, the median total cost (hospital, surgeon, anesthesia) ranges from $30,000 to $50,000. Canada's public system covers most of it, with out-of-pocket expenses limited to medications and supplies.
Insurance coverage and out-of-pocket tips
Most major insurers, including Medicare, classify ulcerative colitis surgery as medically necessary when documented medication failure exists. Preauthorization paperwork is crucialwork with your hospital's financial counselor to avoid surprise bills.
Hidden costs
Don't forget stoma supplies (if you end up with an ileostomy), routine colonoscopies, and potential medication for pouchitis. A budgeting worksheet can help you plan for these recurring expenses.
Cost comparison table
| Option | Upfront Cost | Typical Ongoing Cost | Notes |
|---|---|---|---|
| J-pouch | $30$45k | Medications for pouchitis (if needed) | Potential for higher long-term quality of life |
| Permanent ileostomy | $25$40k | Stoma supplies ($150$300/month) | Predictable expenses |
| Surgery without pouch | $28$42k | Variable, depends on follow-up surgeries | Chosen for specific medical reasons |
Pros & Cons
Decision-making toolkit
We've boiled it down to a simple pros-and-cons list. Use it to weigh what matters most to youwhether it's freedom from daily medication, fear of an external bag, or the possibility of pouchitis.
| Pros | Cons |
|---|---|
| Potential cureUC can't recur after the colon's gone. | Risk of pouchitis (1530%). |
| Many patients achieve normal continence with a J-pouch. | Longer initial recovery than an ileostomy. |
| Often eliminates the need for lifelong steroids or biologics. | Possible pelvic floor dysfunction. |
| No permanent external bag if a pouch is created. | May require a second surgery if pouch fails. |
How to choose the right option
Ask yourself: Am I comfortable managing a stoma? Do I want to avoid an external appliance at all costs? How important is a quick recovery? Discuss these answers with a gastroenterologist and a high-volume colorectal surgeon; their guidance will be personalized to your anatomy and lifestyle.
Preparing for Surgery
Preoperative medical optimization
Good nutrition, quitting smoking, and getting up to date on vaccinations (flu, COVID-19, pneumococcal) reduce complications. Some centers recommend a high-protein diet for two weeks pre-op to boost healing. If you have concerns about related digestive issueslike constipation around proceduresask your team about strategies such as pelvic floor therapy and safe remedies.
Choosing an experienced surgical team
Look for surgeons who have performed at least 50 ulcerative colitis resections and who routinely use laparoscopic or robotic techniques. A proficient team means shorter operative times, less blood loss, and smoother recovery.
Mental-health prep and support groups
Facing surgery can be emotionally taxing. Connecting with peers through the Crohn's & Colitis Foundation's online forums or local support groups can provide comfort, practical tips, and a sense of community.
Preop checklist
- Complete blood work (CBC, CMP, iron studies).
- Colonoscopy to map disease extent.
- Nutrition consult aim for 1.5g protein/kg body weight.
- Stop smoking at least 4 weeks before surgery.
- Arrange a postop caregiver for the first week.
Conclusion
Ulcerative colitis surgery is a major decision, but it also offers a realistic chance at long-term remission and a life less dominated by flare-ups. Success rates are high, especially when performed by an experienced surgeon using minimally invasive methods. The journey does involve riskspouchitis, possible reoperations, and a recovery period that can feel demandingbut with proper preparation, clear expectations, and solid support, many patients find their post-surgery life rewarding and empowering.
If you're standing at that crossroads, talk openly with your gastroenterology team, ask for a second opinion if needed, and consider joining a patient community to hear real stories. And heyif you have questions or want to share your own experience, drop a comment below. Let's navigate this together.
FAQs
When is surgery recommended for ulcerative colitis?
Surgery is recommended when medications fail to control severe flare-ups, or when there's a risk of dysplasia or colon cancer, and quality of life deteriorates.
What are the common types of ulcerative colitis surgery?
The main types are proctocolectomy with J-pouch (ileal pouch-anal anastomosis), total colectomy with permanent ileostomy, and subtotal colectomy without pouch creation.
What is the success rate of ulcerative colitis surgery?
J-pouch surgery has a 90-95% long-term remission rate with many patients living symptom-free after surgery.
What are the risks and complications associated with surgery?
Short-term risks include bleeding, infection, and leaks. Long-term, 15-30% of J-pouch patients may develop pouchitis; other risks include pelvic sepsis or pouch failure.
How long is the recovery after ulcerative colitis surgery?
Hospital stay is typically 2 to 7 days depending on the surgery type, with a return to light activities in 4-6 weeks and full recovery around 8-12 weeks.