Got a diagnosis of stomach cancer and the doctors are throwing around T3N2M0 like its a secret code? Lets cut right to the chase: the 8thedition AJCC TNM system tells you three thingshow deep the tumor has grown (T), whether nearby lymph nodes are involved (N), and if the disease has jumped to distant parts of the body (M). Those three letters and numbers dictate everything from the treatment plan to the odds of longterm survival.
In the next few minutes well break down each piece of the puzzle, highlight whats new in the 8th edition, and give you practical tips you can actually use when you sit down with your radiologist, pathologist, or oncologist. Think of this as a friendly chat over coffeeno jargon, just the facts you need to feel empowered.
Why the 8th Edition?
What changed from the 7th?
The AJCC (American Joint Committee on Cancer) released the 8th edition in 2017 to make staging more precise. The biggest shifts are:
- Refined Tcategories: The old T1 split into T1a (lamina propria/muscularis mucosa) and T1b (submucosa), while T4 now distinguishes between serosal penetration (T4a) and invasion of adjacent organs (T4b).
- Node count matters: Instead of N1 = any nodal involvement, the new system grades N1 (12 nodes), N2 (36 nodes) and N3a (715 nodes) and N3b (16 nodes). This granularity better predicts outcomes.
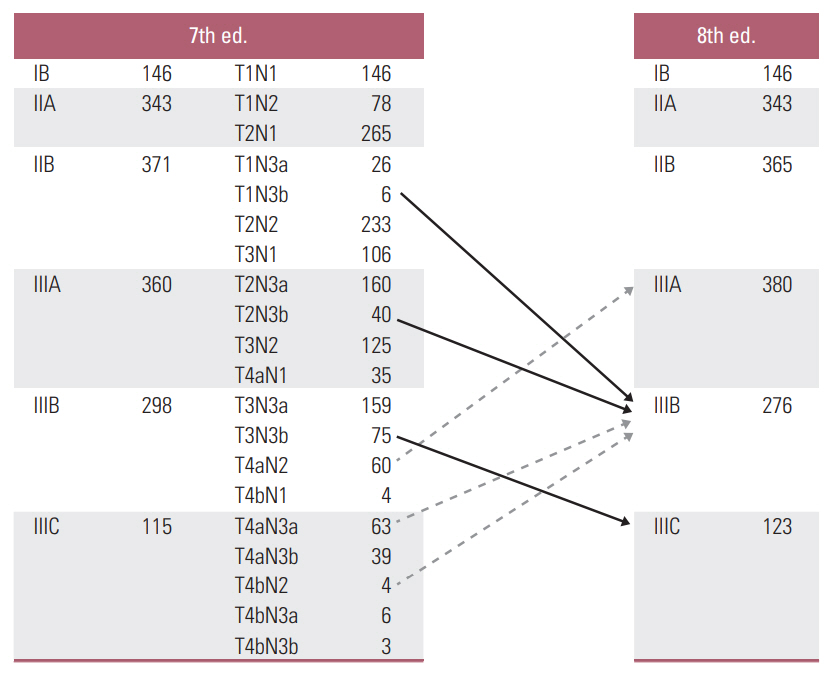
- New stage III subgroups: By combining the updated T and N categories, clinicians can now separate IIIA, IIIB, and IIIC, giving a clearer picture of prognosis.
Why does this matter to you? Because a more nuanced stage means a treatment plan thats less onesizefitsall and more tailored to your specific disease burden. A study of over 3,000 patients showed that the 8thedition staging improved survival prediction by nearly 12% compared with the 7th edition ().
Understanding the T Component
Tstage table
| TLevel | Definition (8thEdition) | Typical Imaging Modality |
|---|---|---|
| TX | Primary tumor cannot be assessed | |
| T0 | No evidence of primary tumor | |
| T1a | Invades lamina propria or muscularis mucosa | Endoscopic ultrasound (EUS) |
| T1b | Invades submucosa | EUS, highresolution CT |
| T2 | Invades muscularis propria | CT or MRI |
| T3 | Invades subserosa | CT |
| T4a | Penetrates serosa (visceral peritoneum) | CT, MRI |
| T4b | Invades adjacent structures (pancreas, liver, etc.) | MRI, PETCT |
Radiology tips
When you look at your scan report, ask the radiologist to point out the exact layer of invasion. Small differencessay, submucosa vs. muscularis propriacan shift you from a T1b to a T2 classification, which often means a move from endoscopic resection to a fullstomach gastrectomy.
Understanding the N Component
Nstage table
| NLevel | Number of Metastatic Nodes | Clinical Significance |
|---|---|---|
| N0 | 0 nodes | Lowest recurrence risk |
| N1 | 12 nodes | Often surgery alone is sufficient |
| N2 | 36 nodes | Typically combined with perioperative chemotherapy |
| N3a | 715 nodes | Consider intensified systemic therapy |
| N3b | 16 nodes | Usually classified as stageIV disease |
Pathology insights
Surgeons aim for a D2 lymphadenectomyremoving at least 15 nodesto ensure accurate staging. If the final pathology shows more nodes than were seen on imaging, thats upstaging, and your treatment plan may become more aggressive. Conversely, understaging can happen when microscopic disease slips past the surgical net, which is why multidisciplinary tumor boards are essential.
Understanding the M Component
What does M0 vs M1 mean?
M0 means no distant spreadyour cancer is confined to the stomach and regional nodes. M1 indicates metastasis to distant organs such as the liver, lungs, or peritoneum. In the 8th edition, any peritoneal carcinomatosis is automatically M1.
Imaging pearls
For suspected M1 disease, a PETCT can pick up metabolically active lesions that a standard CT might miss. However, peritoneal implants often require diagnostic laparoscopy for confirmationsomething your surgeon will discuss if the imaging is equivocal.
Putting It All Together
Stage groupings
Heres a quick look at how the T, N, and M pieces combine into the final stage. Think of it as solving a puzzle where each piece locks into place.
| Stage | T | N | M | Typical 5Year OS* |
|---|---|---|---|---|
| IA | T1ab | N0 | M0 | 90% |
| IB | T2 | N0 | M0 | 80% |
| IIA | T3 | N01 | M0 | 65% |
| IIIB | T34a | N23a | M0 | 45% |
| IIIC | T4b | N3b | M0 | 30% |
| IV | Any | Any | M1 | <10% |
*Overall survival percentages are drawn from NCCNbased cohort studies ().
How stage guides treatment
StageI: often surgery alone (possibly endoscopic resection for T1a).
StageIIIII: multimodalneoadjuvant chemotherapy surgery adjuvant therapy.
StageIV: systemic therapy, palliative radiotherapy, or clinical trials.
Balancing Benefits and Risks
Why staging matters
Accurate staging lets you and your care team choose a regimen that maximizes cure chances while minimizing unnecessary toxicity. It also gives you a realistic expectation of outcomes, which can be a huge emotional relief.
Potential pitfalls
Staging isnt infallible. Imaging can miss micrometastases, and biopsies may not capture the deepest invasion. Overreliance on a single modality can lead to understaging, while aggressive staging procedures can cause anxiety. The key is a balanced, multidisciplinary approachradiology, pathology, surgery, and medical oncology all speaking the same language.
Practical Tools and Resources
How to read reports
When you get your radiology or pathology report, keep a small checklist handy:
- Exact Tcategory (e.g., T3 vs. T4a)
- Number of positive nodes and total nodes examined
- Presence of M0 or any mention of distant lesions
- Margins status if surgery was performed
Checklists and calculators
There are free online calculators (e.g., the AJCC staging app) that let you plug in T, N, and M values to instantly see your stage and suggested treatment pathways. Download a printable version and keep it on your bedside tableknowing is power.
Conclusion
The 8thedition TNM staging system for gastric cancer is more than a collection of letters and numbers; its a roadmap that guides every decision from the operating room to the chemotherapy suite. By understanding what each component means, recognizing the updates that make staging more precise, and using practical tools to interpret your reports, you can engage in informed conversations with your healthcare team and feel a little more in control of a scary journey.
Remember, youre not alonedoctors, nurses, radiologists, and countless patients have walked this path before you. If anything feels overwhelming, ask your team to break it down step by step. Knowledge, empathy, and a dash of humor can turn a complex medical maze into a navigable road.
For patients concerned about long-term outcomes after major oncologic surgery, resources on prostate removal life expectancy and survivorship can sometimes provide useful perspectives on functional recovery and quality of life after complex operations.