Quick answer: for most adults diagnosed with Tcell acute lymphoblastic leukemia (Tcell ALL), the fiveyear overall survival hovers around 3040%, and roughly 60% stay cancerfree at three years. Those numbers can swing dramatically depending on age, genetic markers, and the treatment path you choose.
Why does this matter? Knowing the realistic odds, the factors that tip the balance, and the options on the table helps you (or a loved one) make informed, confident decisions about therapy, followup, and qualityoflife planning. Lets walk through what the data say, what doctors look for, and how you can stay proactive.
What Is Tcell ALL
Definition and Cell Origin
Tcell ALL is a fastgrowing cancer that starts in immature Tlymphocytes, the whiteblood cells that normally mature in the thymus. When these cells go rogue, they spill into the blood and bone marrow, crowding out healthy blood cells.
How Common Is It in Adults?
Adult ALL itself is rare, and Tcelltype makes up about 15% of those cases. Thats why you may not hear it mentioned as often as Bcell ALL, but the stakes are just as high.
Quick Fact Box
- Incidence: ~0.3 cases per 100,000 adults per year
- Typical age at diagnosis: 3050years (though it can occur at any adult age)
- Maletofemale ratio: roughly 1.3:1
Survival & Prognosis
What Is the Overall Survival Rate?
Current populationbased studies report a fiveyear overall survival (OS) of 3040% for adults with Tcell ALL. In other words, out of ten people diagnosed, three to four are expected to be alive five years later, assuming they receive contemporary, intensive therapy.
ThreeYear CancerFree Survival
Data from the indicate about 60% of patients achieve remission that lasts three years or more.
How Does It Compare to Bcell ALL?
| Metric | Tcell ALL (Adults) | Bcell ALL (Adults) | Source |
|---|---|---|---|
| 5yr OS | 3040% | 5060% | Blood2023; Cancer.ca2025 |
| 3yr Remission | ~60% | ~70% | LeukemiaRF2025 |
| Relapse within 2yr | 33% | 20% | PubMed2024 |
Does Age Matter?
Age is a major driver. Patients under 45years tend to fare better, with fiveyear OS approaching 45%, while those over 60 often see survival dip below 20%.
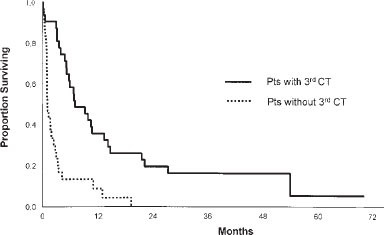
Tcell Leukemia Life Expectancy After Relapse
If the disease returns, median overall survival drops to under 12months. That stark figure underscores how crucial early, effective treatment is.
Factors That Influence
WhiteBloodCell Count at Diagnosis
A high whitebloodcell (WBC) count (above 100k/L) is associated with poorer outcomes. Conversely, lower counts often signal a more favorable response to induction chemotherapy.
Cytogenetics & Molecular Markers
Mutations inNOTCH1 orFBXW7 are considered goodrisk, nudging the fiveyear OS a few points higher. On the flip side, loss ofPTEN or complex karyotypes tend to lower survival chances.
Early Response to Induction (MRD Status)
Patients who become MRDnegative (meaning no measurable residual disease) after the first round of chemo usually see a 15% boost in fiveyear OS. Its a powerful early predictor that doctors track closely.
Coexisting Health Conditions & Performance Status
Overall fitness matters. The ECOG performance scale (0=fully active, 4=completely disabled) strongly correlates with how well a patient tolerates intensive regimens. For example, a 52yearold man with an ECOG of2 and a WBC of 110k/L might only have a ~25% chance of fiveyear survival.
RealWorld Snapshot (Anonymized)
John, a 48yearold accountant, was diagnosed with highrisk Tcell ALL. His WBC was 120k/L, and his cytogenetics showed a NOTCH1 mutation. After a fierce induction phase, he achieved MRDnegative status and went on to an allogeneic stemcell transplant. Five years later, hes celebrating a cancerfree anniversarya story that illustrates how a blend of biology and treatment can rewrite the odds.
Tcell vs Bcell
Survival Differences at a Glance
While both subtypes are forms of ALL, Bcell disease generally flaunts higher survival numbers and a slightly lower relapse rate. That said, Tcell ALL patients often benefit from therapies tailored to Tcell biology, such as nelarabine.
Are Treatment Approaches the Same?
Theres overlapboth groups receive intensive multiagent chemotherapybut Tcellspecific drugs (like nelarabine) and emerging immunotherapies (CART targeting CD7) are uniquely effective for the Tcell variant.
Which Subtype Relapses More Often?
Statistics show Tcell ALL relapses in about onethird of patients within the first two years, compared with roughly onefifth for Bcell ALL. The higher relapse risk partly drives the push for early transplant or clinicaltrial enrollment.
Treatment Options
Standard Intensive Chemotherapy
Regimens such as hyperCVAD (cyclophosphamide, vincristine, doxorubicin, dexamethasone) remain the backbone of frontline therapy. They aim to push the disease into remission quickly, but they also carry significant toxicitiesthink nausea, infections, and temporary hair loss.
Targeted Agents for Tcell ALL
Approved drugs like nelarabine exploit a vulnerability in Tcell nucleoside metabolism, offering an extra punch after standard chemo. Research into BCL2 inhibitors and CD7directed CART cells is also heating up, promising more precise attacks with fewer collateral damages.
Allogeneic StemCell Transplant (SCT)
If youre deemed highrisk (e.g., poor cytogenetics or MRDpositive after induction), an allogeneic SCT can lift fiveyear OS toward 50%. The transplant replaces your diseased marrow with healthy donor cells, offering a potential curebut it also brings risks like graftversushost disease.
Clinical Trials & Emerging Therapies
Participating in a trial can give access to cuttingedge drugs before theyre widely available. For instance, several ongoing studies evaluate CD7CART and bispecific Tcell engagers for adult Tcell ALL. If youre curious, ask your oncologist about enrollingsometimes the best hope lies beyond standard protocols.
Quick Checklist: Is a Clinical Trial Right for You?
- Do you have a clear diagnosis and stable performance status?
- Are you comfortable with additional monitoring and potential sideeffects?
- Is the trials primary endpoint aligned with your personal goals (e.g., longer survival vs. quality of life)?
Relapse & Followup
How Common Is Relapse?
About 33% of adult Tcell ALL patients experience a relapse within the first 12years after achieving remission. Early detection is key.
Options After Relapse
Salvage chemotherapy, a second allogeneic transplant, or enrollment in a CART trial become the mainstays. Unfortunately, outcomes after relapse remain modest, with overall survival lingering under 25%.
Monitoring After Remission
Regular bonemarrow aspirates, flowcytometry for minimal residual disease (MRD), and periodic imaging (CT or PET) form the surveillance backbone. Most oncologists schedule MRD testing every 34months during the first two years, then spaced out as the patient stays diseasefree.
Sample Followup Schedule
| Time Point | Tests | Purpose |
|---|---|---|
| Month3 | Bonemarrow + MRD | Assess induction success |
| Month6 | CT scan + MRD | Check for early relapse |
| Month12 | Bonemarrow + MRD | Confirm continued remission |
| Year23 | Every 6months: MRD, CBC | Longterm surveillance |
| Year45 | Annual CBC + physical | Routine health check |
Sources & Further Reading
For anyone who wants to dig deeper, the following sources back up the numbers and recommendations presented here:
- Management of adults with Tcell lymphoblastic leukemia Blood (2023)
- LeukemiaRF TCell Lymphoblastic Leukemia Overview (2025)
- Cancer.ca Prognosis & Survival Data (2025)
- StatPearls Adult TCell Leukemia (2024)
- PubMed Relapse and salvage outcomes (2024)
Conclusion
Facing a Tcell ALL diagnosis can feel like stepping into a storm, but the picture isnt all dark. Survival rates are modestroughly 3040% at five yearsbut theyre improving thanks to targeted drugs, better transplant techniques, and innovative immunotherapies. Understanding the factors that sway the oddsage, genetics, early responseand staying engaged with your care team can tilt the balance in your favor.
If you or someone you love is navigating this journey, talk openly with your oncologist about the newest treatment options, consider clinicaltrial participation, and keep a close eye on followup testing. Knowledge, support, and proactive care are powerful allies. Youre not alone, and hope is very much part of the equation.
For information on related cancer prognosis topics, some readers also find practical guidance on prostate cancer outlook useful when comparing treatment planning and longterm followup approaches across cancer types.
FAQs
What is the typical five-year survival rate for adults with T-cell ALL?
Adults diagnosed with T-cell acute lymphoblastic leukemia typically have a five-year overall survival rate of approximately 30 to 40%, depending on treatment and individual factors.
How does age affect the prognosis of T-cell ALL in adults?
Patients under 45 years tend to have better outcomes with around 45% five-year survival, while those over 60 may see survival drop below 20%.
What role do genetic markers play in T-cell ALL prognosis?
Mutations like NOTCH1 and FBXW7 are associated with better prognosis, slightly increasing survival chances, whereas loss of PTEN or complex karyotypes tend to worsen outcomes.
What treatment options improve T-cell ALL prognosis in adults?
Standard intensive chemotherapy combined with targeted agents like nelarabine and allogeneic stem cell transplant for high-risk patients can improve survival rates.
How common is relapse in adult T-cell ALL, and what happens after relapse?
About one-third of adults with T-cell ALL experience a relapse within the first two years of remission; outcomes after relapse are poor, with median survival under 12 months and limited effective salvage options.