Quick Answer
What is supine hypertension in Parkinsons? Its a rise in blood pressure that shows up when someone with Parkinsons lies flat, often alongside orthostatic hypotension (the dizzylowBP feeling when standing.
Why should you care? Unchecked, it can increase the risk of stroke, heart problems, and disturb sleep. The good news? Simple monitoring and a balanced treatment plan can keep it under control. If you need help navigating insurance or assistance programs for specific Parkinsons treatments, resources like Exondys 51 assistance can offer guidance on patient support options.
What Is SH?
Definition & Thresholds
Supine hypertension (SH) is defined as a systolic/diastolic blood pressure150/90mmHg after at least five minutes lying flat, or a rise of20mmHg from standing to supine. The condition is part of the broader autonomic dysregulation seen in many people with Parkinsons disease.
QuickReference Table
| Position | Normal BP | SH Threshold |
|---|---|---|
| Supine (5min) | <130/80mmHg | 150/90mmHg |
| Standing | <120/80mmHg | Drop20mmHg from supine |
How It Differs From Regular Hypertension
Regular high blood pressure stays elevated throughout the day, no matter how youre positioned. SH, by contrast, spikes only when youre lying down and may even normalize when you sit or stand. That flipflop can make it tricky to spot unless you purposely measure your supine reading.
How Common?
Prevalence Numbers
Research shows that 3050% of Parkinsons patients who already have neurogenic orthostatic hypotension (OH) also develop SH (see a review in Neurology). So, if youre already dealing with OH, youre definitely in the higherrisk camp.
Whos At Higher Risk?
Longer disease duration, severe autonomic failure, and a nondipping nighttime BP pattern all raise the odds. In everyday language: the longer youve been living with Parkinsons, the more likely your nervous system will scramble the bloodpressure controls.
RealWorld Example
John, a 68yearold retired carpenter, noticed his caregivers BP cuff read 165/95mmHg every night after he turned over in bed. Hed never felt high during the day. After a simple supine BP check, his neurologist diagnosed SH, and his treatment plan changed dramatically.
Symptoms & Red Flags
Typical Symptoms
- Morning headaches that feel pressurelike
- Blurred vision when you roll over
- Dizziness that actually gets worse after youve been lying down for a while
- Nocturnal sweating or feeling hot under the covers
When to Seek Urgent Care
If you ever experience sudden chest pain, an intense pounding headache, or any sign that could indicate a stroke, call emergency services right away. Supine hypertension can be silent, but when it spikes dramatically, the stakes rise quickly.
SymptomChecklist (Downloadable)
Weve prepared a printable PDF you can keep by the bedside. It lists the signs above and lets you tick them off each night. , keeping a symptom log improves communication with your care team.
Why Does SH Happen?
Neurogenic Mechanisms
The brains baroreflexlike a thermostat for blood pressuregets damaged in Parkinsons. When you lie flat, blood pools in the central circulation, and the failing reflex can overcompensate, sending an extra surge of norepinephrine that pushes the pressure upward.
Medication Contributors
Some Parkinsons meds, especially levodopa and certain MAOB inhibitors, can inadvertently raise supine BP. Even a bloodpressure medication meant for OH, such as midodrine, may need careful timing so it doesnt pop up your nighttime numbers.
Other Contributing Factors
- Sleep apneaintermittent breathing pauses spike BP.
- Kidney dysfunctionlimits the bodys ability to regulate fluid balance.
- Dehydrationmakes the cardiovascular system overreact when you finally lie down.
MiniInfographic Idea
Picture a simple flowchart: Brain Baroreflex Norepinephrine Blood Vessels Supine BP. It helps visual learners see the chain reaction.
SH OH Relationship
TwoSided Coin
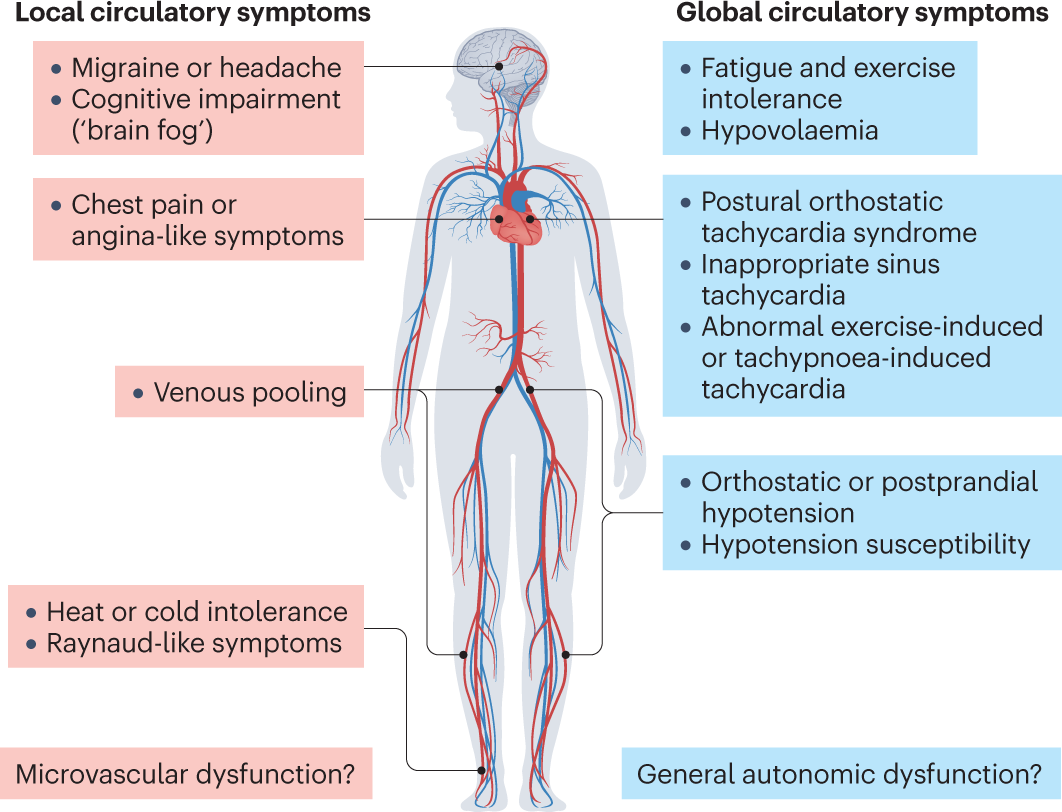
Think of SH and OH as the yin and yang of bloodpressure control in Parkinsons. When you stand, the autonomic nerves cant keep the vessels tight enough, leading to low BP (OH). When you lie down, the same faulty system can overtighten, causing high BP (SH). Both are symptoms of the same underlying imbalance.
Clinical Implications
Because the two conditions counteract each other, treatment must walk a tightrope: raise standing pressure enough to stop dizziness, but not so much that your nighttime BP rockets. Thats why onesizefitsall approaches rarely work.
Comparison Table
| Goal | SH Priority | OH Priority |
|---|---|---|
| Medication Timing | Take meds early in the day | Consider lowdose bedtime meds |
| Bed Position | Headup tilt (1015cm) | Avoid excessive headup tilt |
| Fluid Intake | Limit fluids 12h before bed | Steady hydration throughout day |
How to Diagnose SH
Practical BP Measurement Protocol
- Have the patient lie flat for five minutes in a quiet room.
- Record the blood pressure immediately, then again after the full five minutes.
- Repeat the measurement at night using an ambulatory BP monitor or a home cuff that can log supine readings.
- Document the numbers and bring them to your neurologist or cardiologist.
Useful Tools & Apps
There are a handful of validated ambulatory BP monitors that sync with smartphone apps, allowing you to track trends over weeks. Look for devices that specifically mention a supine mode theyre built for cases like this.
StepbyStep Video Script Idea
If youre a visual learner, imagine a short video where a caregiver shows how to place the cuff, tilt the bed, and record the numbers. You could even record yourself for your own reference.
Treatment Options
NonPharmacologic Strategies
- Elevate the head of the bed 1015cm (a wedge pillow works well).
- Avoid large fluid loads within two hours of bedtime.
- Wear loosefitting clothing; tight belts can worsen bloodpooling.
Pharmacologic Options
| Drug | Typical Dose | How It Works | Key Caution for PD |
|---|---|---|---|
| Midodrine | 2.510mg three times daily | Alpha1 agonist constricts vessels, raising standing BP | May increase supine pressure; use with bedtime headup tilt |
| LDOPS (Droxidopa) | 100600mg three times daily | Boosts norepinephrine production | Monitor supine BP closely |
| Clonidine (lowdose) | 0.05mg at night | Central 2agonist lowers supine BP | Can drop standing BP; adjust timing |
Emerging Therapies
Researchers are experimenting with nitricoxide donors and even renal denervation to temper the extreme swings, but those are still in trial phases. Keep an eye on clinicaltrial registries if youre interested in cuttingedge options.
PatientCase Flowchart
A simple flowchart can guide you: Start with lifestyle check supine BP add lowdose midodrine if standing BP still low consider nighttime clonidine if supine BP stays high. Visualizing the steps keeps you from feeling overwhelmed.
Lifestyle & HomeCare Tips
Bedtime Positioning
Use a wedge pillow or a folded blanket under the mattress to keep your head slightly elevated. Its a small change that can lower supine pressure by up to 15mmHg.
Diet & Hydration
Salt isnt the enemy here a modest salty snack before bed (think pretzels or olives) can help keep your blood volume up while youre upright. Throughout the day, sip water consistently rather than gulping large amounts all at once.
Monitoring Routine
Pick a quiet time each morning, lie flat for five minutes, and record your BP. Do the same right before you get out of bed at night if you have a monitor that can log supine readings. Share the log with your neurologist every few months. If insurance coverage for frequent outpatient testing or devices is a concern, see resources about Exondys 51 insurance as an example of how patient advocacy sites outline coverage and assistance pathways for specialized neurology therapies; similar approaches may help with BP monitoring devices.
Printable BPLog Template
Weve created a simple table you can print and fill in. It asks for date, time, supine systolic, supine diastolic, standing systolic, standing diastolic, and any symptoms you noticed. Consistency is the secret sauce.
Bottom Line
Supine hypertension is a common but often overlooked companion to orthostatic hypotension in Parkinsons disease. By checking your blood pressure while youre lying down, using a balanced mix of headup tilt, modest lifestyle tweaks, andwhen neededcarefully timed medication (like midodrine or lowdose clonidine), you can keep those nighttime spikes from turning into serious cardiovascular events.
Talk to your neurologist or an autonomic specialist about getting a supine BP log started today. Download the free checklist, share your experience in the comments, and lets keep each other informed. Your health journey doesnt have to be a solitary climb were in this together.
FAQs
What is supine hypertension in Parkinson’s disease?
Supine hypertension in Parkinson’s is a condition where blood pressure rises significantly when a person lies flat, often accompanied by orthostatic hypotension, due to autonomic nervous system dysfunction.
How common is supine hypertension among Parkinson’s patients?
It occurs in about 30–50% of Parkinson’s patients who have neurogenic orthostatic hypotension, particularly in those with longer disease duration and more severe autonomic failure.
What symptoms indicate supine hypertension in Parkinson’s?
Symptoms may include morning headaches, blurred vision upon rolling over, worsening dizziness after lying down, and nocturnal sweating. Sometimes it causes no obvious symptoms but can still increase cardiovascular risk.
How is supine hypertension diagnosed in Parkinson’s patients?
Diagnosis involves measuring blood pressure after lying flat for five minutes, ideally using ambulatory or home BP monitors with supine mode, and noting if BP is ≥150/90 mmHg or rises ≥20 mmHg from standing to supine.
What treatments are available for supine hypertension in Parkinson’s?
Treatment includes lifestyle changes like elevating the head of the bed, limiting fluids before bedtime, and carefully timed medications such as midodrine or low-dose clonidine to balance supine and standing blood pressure.