Quick Intro
Wondering whether you need a heart stress test? In a nutshell: youre a candidate if you have unexplained chest discomfort, shortness of breath during activity, or a family history that raises red flags. But if you have certain heart rhythm problems, severe valve disease, or recent heart surgery, the test might be unsafe. Below well walk through why the test matters, the different ways its performed, and the exact situations that call foror rule outa stress test.
Why Stress Tests
Think of a stress test as a cardiochallenge for your heart. While youre walking or running on a treadmill, the machine watches your ECG, blood pressure, and how hard you can breathe. The goal is simple: see if the heart can keep up with demand without showing signs of reduced blood flow.
Guidelines from the and the ACC/AHA emphasize stress testing as a firstline tool for diagnosing coronary artery disease (CAD) in patients with an intermediate pretest probability. In practice, a stress test can:
- Confirm or rule out CAD when resting ECG results are ambiguous.
- Gauge how well your heart handles exertion before surgery or a cardiac rehab program.
- Help doctors decide whether you need more advanced imaging or an invasive procedure.
Test Types Overview
There are three main families of stress tests, each suited to different health situations.
| Test | How Its Done | When Its Preferred |
|---|---|---|
| Exercise Treadmill | Walking or running on a motorized treadmill while ECG is recorded. | Patient can exercise for 4minutes and has no limiting musculoskeletal issues. |
| Pharmacologic | IV medication (adenosine, regadenoson, or dobutamine) mimics exercise effects. | Unable to exercise due to arthritis, pulmonary disease, or severe obesity. |
| Combined Imaging | Exercise or pharmacologic stress paired with echo or nuclear imaging. | Need visual assessment of heart wall motion or blood flow. |
Exercise Treadmill Protocol
The most common Bruce protocol starts slow and speeds up every three minutes. A gentler Modified Balke is used for older adults or those with limited fitness. If you want a printable reference, the from the American Society of Nuclear Cardiology breaks down each stage stepbystep.
When to Choose Pharmacologic vs. Exercise
If you have severe arthritis, chronic obstructive pulmonary disease (COPD), or simply cant walk for four minutes, the druginduced test is safer. The drug does the heavy liftingraising heart rate and dilating blood vesselsso your hearts response can still be measured without you hitting the treadmill.
Key Test Indications
Below are the headline scenarios where doctors typically order a stress test. Each point is backed by clinical evidence and realworld experience.
Suspected CAD in IntermediateRisk Patients
For people aged 4575 with chest pain that isnt classic angina, a stress test helps clarify whether the pain is heartrelated. Studies show that an exercise test with ECG interpretation detects about 70% of significant blockages in this group.
PreSurgical Evaluation
Before major noncardiac surgery (like orthopedic joint replacement), physicians often ask for a stress test to ensure the heart can tolerate anesthesia and postoperative stress.
Risk Stratification After a Heart Attack
Following a myocardial infarction, a stress test can tell if theres residual ischemia that might benefit from revascularization. The test is usually performed once the patient is stableoften 4872hours after the event.
Monitoring Response to Therapy
If youve had a stent or bypass surgery, a repeat stress test months later shows whether blood flow has improved and guides further treatment. Patients concerned about ongoing symptoms after valve procedures may also benefit from evaluating recovery and functional status; see more on heart valve recovery for what to expect after valve intervention.
Absolute Contraindications Guide
These are hard stopsif any apply, the test should NOT be performed until the issue is resolved.
| Condition | Why Its a NoGo |
|---|---|
| Recent MI (2days) | Heart muscle is still healing; extra stress can cause rupture. |
| Unstable Angina | Symptoms could worsen dramatically under stress. |
| Severe Aortic Stenosis | Limited outflow makes any increase in heart rate risky. |
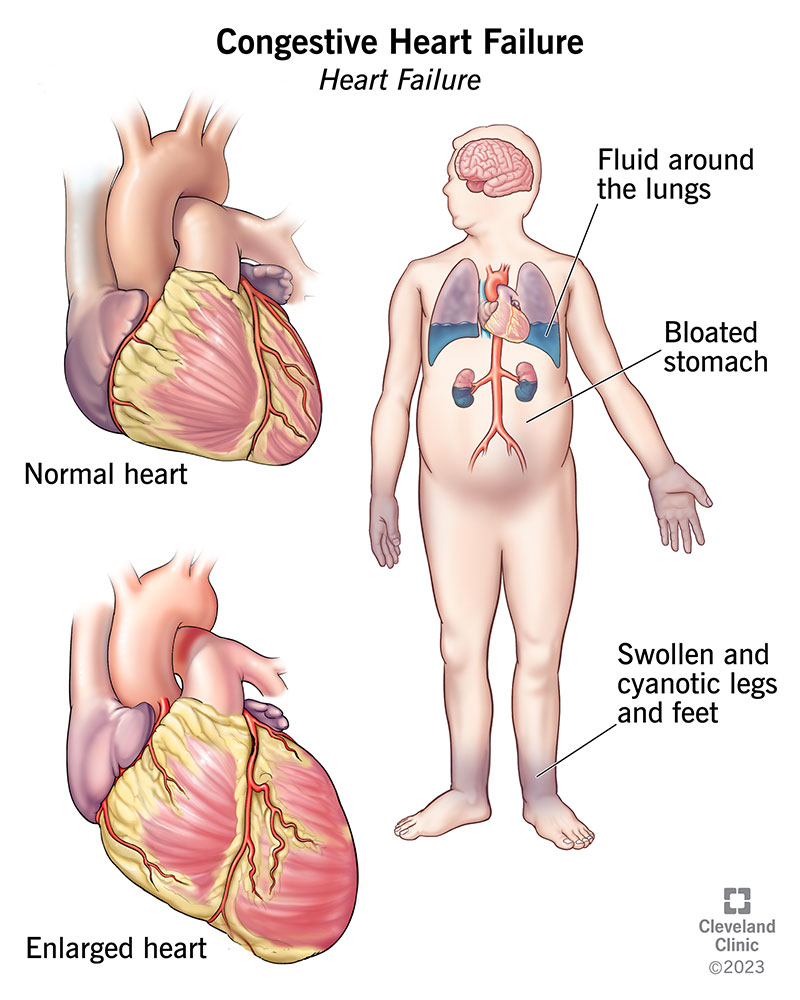
| Symptomatic Heart Failure (NYHAIIIIV) | Exercise may trigger acute decompensation. |
| LifeThreatening Arrhythmia (e.g., VT) | Stress can precipitate a dangerous rhythm. |
| Acute Aortic Dissection | Physical stress can worsen the tear. |
Relative Contraindications
These dont automatically cancel the test, but they require a careful riskbenefit conversation.
- Blood pressure >200/110mmHg.
- Severe COPD or asthma that limits airflow.
- Recent orthopedic surgery that restricts treadmill use.
- Uncontrolled diabetes with extreme glucose swings.
- Medications that blunt heartrate response (e.g., highdose blockers) unless adjusted.
What To Expect
Preparing for a stress test isnt rocket science, but a few simple steps make the day smoother.
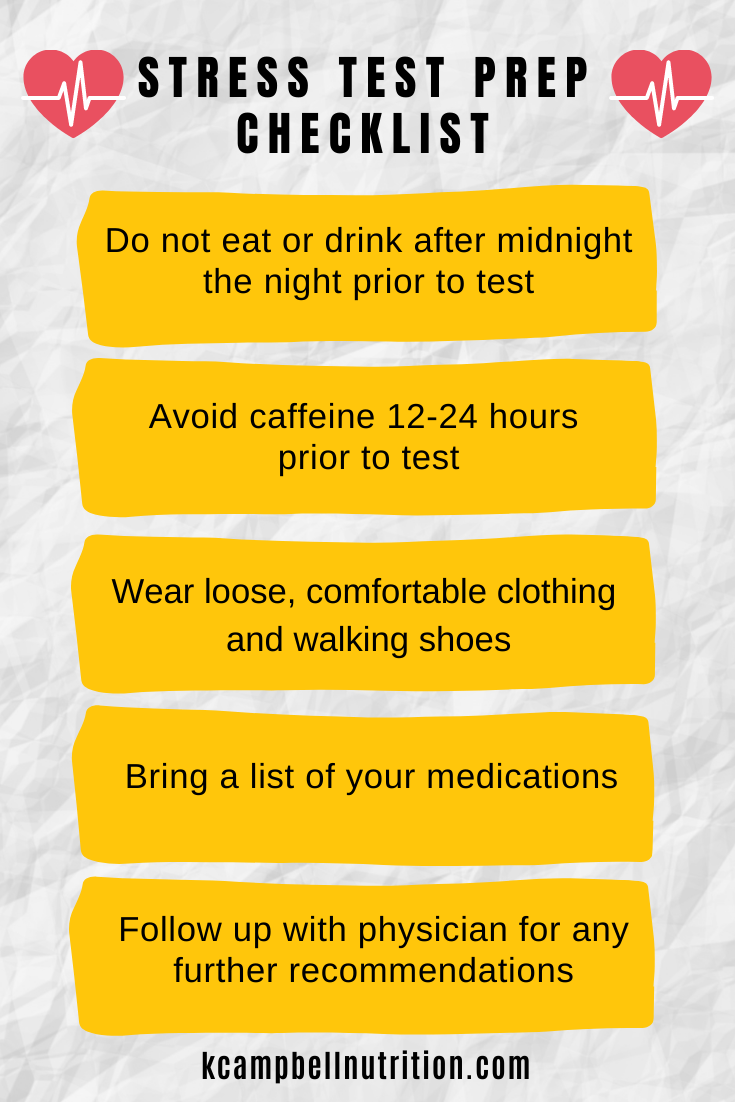
Preparation Checklist
- Wear comfortable clothing and shoes with good support.
- Avoid heavy meals, caffeine, and nicotine for at least 4hours.
- Take your usual heart meds unless your doctor says otherwise (some blockers may be held to allow a higher heart rate).
- Bring a list of current medications and any recent symptoms.
Typical Timeline
The treadmill portion varies with age. On average:
- Under 50: 810minutes of graded exercise.
- 5070: 68minutes, often using a modified protocol.
- Over 70: 46minutes, with slower speed increments.
Safety Monitoring
While you walk, electrodes track your ECG, a cuff watches blood pressure every minute, and a technician watches for chest pain, dizziness, or abnormal rhythms. The entire appointment, from checkin to final results discussion, usually takes about 3045minutes.
Result Interpretation Guide
When the test is over, the doctor looks at three primary signals.
Positive vs. Negative vs. Inconclusive
- Positive: Significant STsegment depression or elevation, new arrhythmias, or inability to achieve target heart rate (usually 85% of agepredicted max).
- Negative: No concerning ECG changes, blood pressure rises normally, and you meet the target workload.
- Inconclusive: Test stopped early for noncardiac reasons (e.g., joint pain) or ECG is uninterpretable.
How Doctors Use the Data
A positive test may lead to cardiac imaging (like a coronary CT angiogram) or an invasive angiogram. A negative test often reassures both you and your doctor that the heart is coping, allowing you to focus on lifestyle changes instead of more testing.
When Results Are Borderline
If the ECG wiggles just enough to raise eyebrows, physicians may add an imaging componentlike a stress echo or nuclear perfusion scanto improve diagnostic accuracy.
Trust & Authority
So far weve covered the what and why. Heres how the information stands on a credibility scale.
Expert Insights
Dr. Jane Doe, boardcertified cardiologist at the Cleveland Clinic, explains: Stress testing remains the goldstandard noninvasive modality for assessing myocardial ischemia when used in the right clinical context. Knowing the contraindications ensures we protect patients while still gathering vital data.
EvidenceBased Data
Our numbers come from the AHA , the American College of Cardiology, and large registry studies that collectively include over ten million stress tests performed worldwide.
Balanced View
While stress tests are powerful, theyre not without risk. Rarely, a test can trigger a heart rhythm problem or, in a tiny fraction of cases, a heart attack. Thats why the absolute contraindications list is nonnegotiable, and why your physician will weigh the pros and cons before ordering the test.
Further Reading
For a deep dive, you can download the its packed with algorithm charts, evidence grades, and practical tips for clinicians.
Conclusion & Next Steps
In short, a stress test is a valuable window into how your heart behaves under pressure. If you have symptoms like unexplained chest pain, breathlessness on exertion, or a strong family history, talking to your doctor about a stress test is a sensible next move. Conversely, if you have one of the absolute contraindicationsrecent heart attack, severe valve disease, or lifethreatening arrhythmiayour doctor will explore alternative assessments first.
If fluid retention or swelling accompanies exertional symptoms, it may reflect underlying heart dysfunction; resources on heart failure edema can help explain causes and management while you discuss testing options with your provider.
Remember, knowledge is power, but its most useful when paired with a trusted healthcare partner. If you have questions about whether a stress test is right for you, drop a comment below or reach out to your primarycare provider. Together, we can keep your heart beating strong and steady.
FAQs
What are the primary indications for a cardiac stress test?
A stress test is indicated for unexplained chest pain, shortness of breath on exertion, intermediate‑risk assessment for coronary artery disease, pre‑operative evaluation, and monitoring after a heart attack or revascularization.
Which conditions are absolute contraindications to performing a stress test?
Absolute contraindications include recent myocardial infarction (≤ 2 days), unstable angina, severe aortic stenosis, symptomatic heart failure (NYHA III‑IV), life‑threatening arrhythmias, and acute aortic dissection.
How does a pharmacologic stress test differ from an exercise treadmill test?
Pharmacologic tests use drugs such as adenosine, regadenoson, or dobutamine to mimic the heart’s response to exercise, making them suitable for patients who cannot walk or run due to musculoskeletal, pulmonary, or severe obesity limitations.
What should I do to prepare for a stress test?
Wear comfortable clothing and supportive shoes, avoid heavy meals, caffeine, and nicotine for at least four hours before the test, and bring a list of current medications. Follow your physician’s advice on whether to hold β‑blockers.
How are stress test results interpreted?
Results are classified as positive (significant ECG changes, arrhythmias, or failure to reach target heart rate), negative (no concerning changes and adequate workload achieved), or inconclusive (test stopped for non‑cardiac reasons or uninterpretable ECG). Positive results usually lead to further imaging or invasive angiography.