If youve ever noticed an itchy, red flareup that appears just before your period or after a hormone shot, you might be dealing with a progesterone rash. Its frustrating, but you don't have to endure it in silence.
The good news? Most women find relief with a blend of topical care, hormone tweaks, and lifestyle adjustments. The right plan depends on how severe the rash is, whether youre trying to conceive, and your overall health. Lets walk through what you need to knowno fluff, just clear, friendly guidance.
What Is It?
Definition & Medical Name
The condition is medically called autoimmune progesterone dermatitis (APD) or progesterone hypersensitivity. In short, your immune system reacts to the hormone progesterone, whether its produced naturally or introduced through medication.
How Hormones Trigger the Skin
During the luteal phase of your cycleroughly five to seven days before menstruationprogesterone levels surge. In sensitive individuals, that surge sparks an immune response that shows up as a rash. Think of it as your skin throwing a tiny, unwanted temper tantrum because its been handed a hormone it doesnt recognize.
Visual Guide
Seeing is believing. often display erythematous plaques, urticarial welts, or eczemalike patches that may appear on the face, chest, or limbs. can help you match what youre seeing on your own body.
Who Gets It?
While APD can affect anyone, its most common in women of reproductive ageespecially those using oral contraceptives, undergoing IVF, or receiving progesterone injections. Even if youre not trying to get pregnant, the hormonal swings of a regular cycle can be enough to trigger a flare. If you are pursuing fertility treatments, learning about lean PCOS fertility considerations may also help your care team tailor protocols that minimize hormone-triggered skin reactions.
RealWorld Anecdote
Take Emma, a 32yearold undergoing IVF. After her third progesterone shot, a rash erupted on her neck and spread to her arms within 48 hours. A quick switch to a lowdose GnRH antagonist and a short course of topical steroids cleared the skin in a week, allowing her cycle to continue smoothly.
Spotting the Signs
Typical Skin Patterns
APD usually shows up as bright red, raised patches that can look like hives, eczema, or even tiny pustules. The rash may be localized or cover large areassometimes over 10% of the body surface.
Timing of FlareUps
Most people notice the rash during the luteal phase, but it can also appear shortly after a progesterone injection or during IVF protocols when high doses are used. The key clue is the consistent link to a hormonal event.
Accompanying Signs
Beyond itching and burning, you might experience facial swelling, watery eyes, or a sense of tightness under the skin. If swelling spreads to the lips or throat, seek medical help immediatelythats a sign of a more serious allergic reaction.
Quick SelfCheck Checklist
- Red, itchy patches that appear 57days before your period?
- Rash flares after a progesterone shot or IVF medication?
- Symptoms improve with antihistamines or topical steroids?
Why Does It Happen?
Autoimmune Progesterone Dermatitis
In APD, your immune system mistakenly flags progesterone as an invader. This can involve IgEmediated (allergytype) reactions or delayedtype hypersensitivity, where Tcells orchestrate the skin inflammation.
Contributing Factors
Genetics, a history of allergies, or prior exposure to highdose hormonal therapies can increase the odds. Even certain IVF protocols that flood the body with synthetic progesterone can tip the balance.
Diagram of the HormonalImmune Loop
Imagine a seesaw: on one side sits progesterone, on the other the immune system. When progesterone spikes too high, the immune side tilts, sending out inflammatory signals that land on the skin.
Progesterone Rash Treatment Options
FirstLine Symptomatic Relief
For mild flares, start with topical steroidshydrocortisone 1% for a few days, moving to a midpotency cream like triamcinolone if needed. Pair this with a nonsedating antihistamine such as cetirizine; it can calm itching within hours.
Hormonal Interventions
When the rash is tied tightly to hormonal cycles, adjusting the hormone environment often brings lasting peace.
Oral Contraceptive Pills (OCPs)
Estrogendominant OCPs can suppress the natural progesterone surge, reducing flare frequency. Talk to your provider about a lowdose combined pill that fits your lifestyle.
GnRH Agonists
These drugs (e.g., leuprolide) put a temporary pause on ovulation, essentially turning off the progesterone engine. Theyre powerful but can cause menopausallike symptoms, so theyre usually reserved for moderatetosevere cases.
Tamoxifen & AntiEstrogen Agents
When OCPs arent an optionperhaps due to clotting risktamoxifen can block estrogens effect, indirectly lowering progesterone production.
Progesterone Desensitization
In specialized centers, a stepup protocol exposes you to tiny, gradually increasing doses of progesterone. Over weeks, many patients achieve tolerance, allowing them to continue IVF or hormone therapy without rash recurrence.
Systemic Therapies for Severe Cases
If the skin is widely affected or the rash wont calm down with topical measures, a short course of oral prednisone (typically 0.5mg/kg for five days, then taper) can bring quick relief. Keep an eye on blood sugar and mood changes, thoughsystemic steroids are a doubleedged sword.
Immunomodulators
Emerging evidence suggests omalizumab, an antiIgE monoclonal antibody, can help women with stubborn APD. Its still offlabel, but some dermatologists report promising results.
Natural & Lifestyle Adjuncts
While natural cures alone rarely eradicate the rash, certain habits can tip the scales toward calm skin.
Foods to Avoid
Youve probably heard of autoimmune progesterone dermatitis foods to avoid. Highhistamine itemssuch as aged cheese, fermented soy, and certain nutscan amplify inflammation. Caffeine and alcohol may also heighten hormonal fluctuations, so consider cutting back during luteal days.
AntiInflammatory Diet
Boost omega3 fatty acids (salmon, flaxseed), vitaminD (sunlight, fortified dairy), and probiotics (yogurt, kefir). These nutrients act like peacekeepers, soothing the immune response.
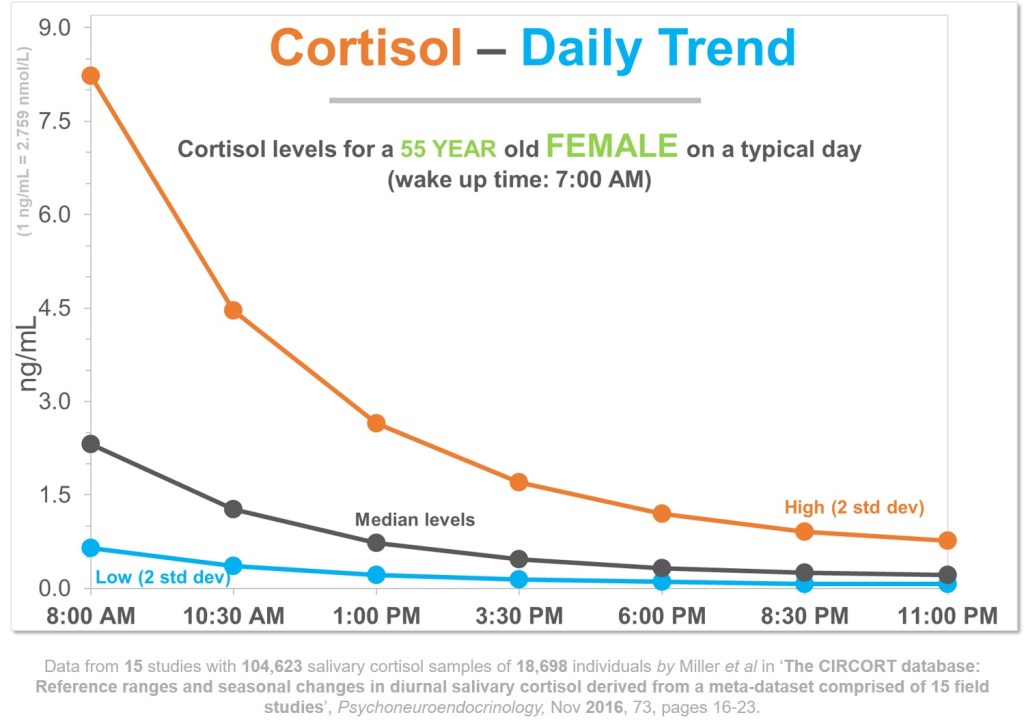
Stress Reduction
Stress releases cortisol, which can paradoxically increase progesterone levels. Simple practicesfive minutes of deep breathing, a short walk, or a calming playlistcan keep your hormonal orchestra in tune.
IVFSpecific Considerations
If youre in the middle of an IVF cycle and a rash appears, you have options.
Adjusting Stimulation Protocols
Many clinics now use antagonist protocols that require lower progesterone doses. Discuss swapping to a gentler regimen with your reproductive endocrinologist.
Managing FlareUps During Embryo Transfer
A brief taper of oral steroids (e.g., prednisone 10mg for 3 days) combined with a topical steroid can keep the rash at bay without compromising embryo implantation.
Diagnostic Workup
Clinical History & Menstrual Correlation
The first step is a detailed diary: note the day of your cycle, any hormonal meds, and rash appearance. This timeline is the compass that guides diagnosis.
Skin Biopsy
Rarely needed, but a punch biopsy can rule out other skin conditions such as psoriasis or contact dermatitis.
Hormone Challenge Testing
Under medical supervision, a tiny intradermal injection of progesterone can provoke a localized reaction, confirming hypersensitivity. Its safe when performed by an experienced allergist.
Allergy Testing
Serum IgE levels or patch tests may reveal whether the reaction is IgEmediated. This information helps decide if omalizumab could be useful.
Diagnostic Algorithm Flowchart
| Step | Action | Result |
|---|---|---|
| 1. Symptom diary | Track rash vs. cycle | Pattern identified? |
| 2. Physical exam | Check for typical lesions | Consistent with APD? |
| 3. Hormone challenge | Intradermal progesterone | Positive reaction confirmed |
| 4. Lab tests | IgE, hormone levels | Guide treatment choice |
TakeHome Checklist
Daily SkinCare Routine
Use a gentle, fragrancefree cleanser, followed by a soothing, hypoallergenic moisturizer. Apply a lowpotency steroid only during flareups and limit use to 710 days.
Medication Log
Document every pill, injection, and overthecounter antihistamine. Note the day of your cycle, rash intensity (110 scale), and any food or stress triggers. This log becomes your personal rashcontrol manual.
Diet & Lifestyle Quick List
- Avoid highhistamine foods (aged cheese, fermented soy, citrus).
- Limit caffeine & alcohol during luteal phase.
- Eat omega3 rich meals 34 times a week.
- Practice 5minute deepbreathing exercises daily.
When to Call Your Doctor
If the rash covers more than 10% of your body, spreads rapidly, or is accompanied by swelling of the lips, throat, or difficulty breathing, seek immediate medical attention. Otherwise, schedule an appointment if the rash persists beyond a week of home treatment.
Conclusion
A progesterone rash can feel overwhelming, but with the right combination of topical care, hormone management, and lifestyle tweaks, most women regain clear skin and keep their fertility plans on track. Talk to a dermatologist or reproductive endocrinologist to craft a personalized progesterone rash treatment plan that respects your body and your goals. If youve tried any of these strategies, share what worked for youyour experience could be the lifeline someone else needs.