At first I thought it was just heartburn until the gnawing pain after each meal wouldnt quit. If youre wondering how doctors actually confirm a prepyloric ulcer, the answer is right here no extra scrolling needed.
Well cut to the chase: the key symptoms, the most reliable tests (including the goldstandard endoscopy), and the safest treatment options, all backed by the latest medical guidelines.
Why prepyloric matters
What is a prepyloric ulcer?
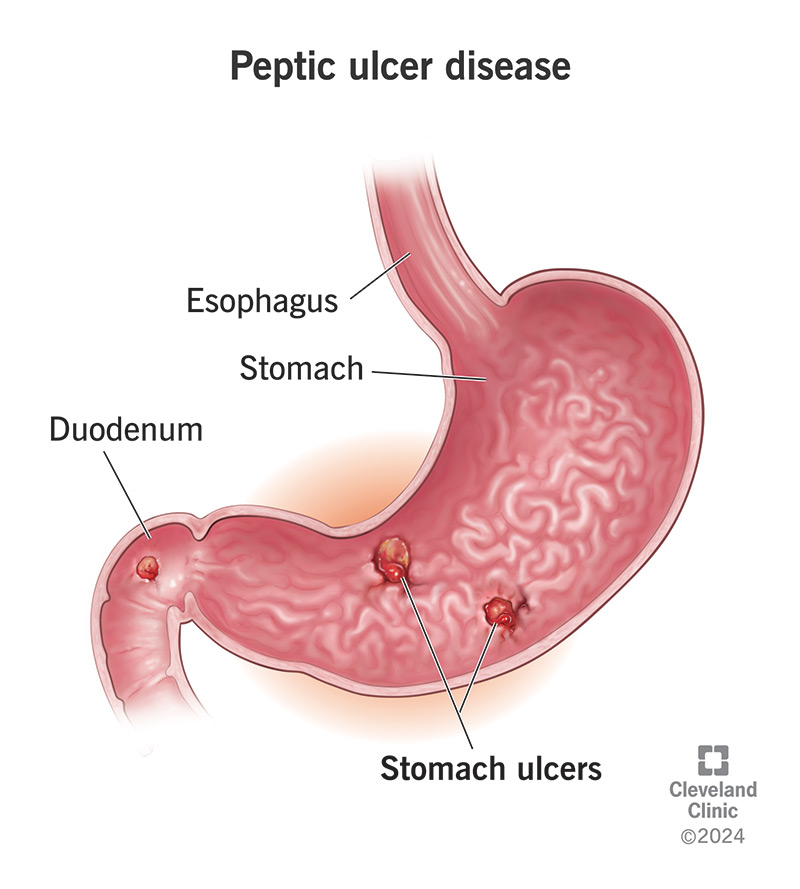
A prepyloric ulcer is a sore that forms just before the pylorus the gateway between your stomach and duodenum. Its technically a gastric ulcer, but its location matters because it sits right where food exits the stomach, often causing that classic fullafterabite feeling.
Common causes
The usual suspects are Helicobacter pylori infection, regular use of nonsteroidal antiinflammatory drugs (NSAIDs), smoking, and chronic stress. According to the Mayo Clinic, H.pylori is responsible for up to 80% of cases, while NSAIDs account for another 1520%.
Whos at risk?
Adults over 40, especially those who take painkillers for arthritis or have a history of smoking, are more prone. Men tend to develop gastric ulcers slightly more often than women, but the gap narrows once H.pylori is in the picture.
Quick fact box
| Statistic | Source |
|---|---|
| 10% of all peptic ulcers are prepyloric | NIDDK |
| H.pylori infection prevalence worldwide: 44% | World Health Organization |
| NSAIDrelated ulcer risk increases 5fold with chronic use | Cleveland Clinic |
Spotting warning signs
Typical symptoms
Most people describe a burning or gnawing ache in the upper abdomen that often improves after eating a little, then returns a few hours later. Nausea, loss of appetite, and an uncomfortable fullness after just a few bites are also common.
Redflag warning signs
If you notice any of these, dont wait:
- Vomiting blood or material that looks like coffee grounds
- Black, tarry stools (a sign of digested blood)
- Sudden, severe abdominal pain that doesnt ease
- Unexplained weight loss of more than 5% in a month
These are the classic answers to what are the warning signs of an ulcer? and signal the need for urgent medical attention.
When symptoms mimic something else
Heartburn, gallbladder disease, and functional dyspepsia can all masquerade as ulcer pain. Thats why a proper workup is essential you dont want to treat the wrong culprit.
Patient story (experience)
Take Jamie, a 42yearold accountant who chalked his afterlunch heaviness up to stress. After three months of worsening pain, a quick visit to his doctor and an endoscopy revealed a 6mm prepyloric ulcer. Treatment lifted his symptoms in just three weeks proof that early diagnosis truly matters.
How doctors confirm
Medical history & physical exam
First, the doctor asks about pain patterns, medication use, and lifestyle habits. During the exam, they may press on the abdomen to check for tenderness. This step helps narrow down the differential diagnosis.
Noninvasive tests
When an ulcer is suspected, doctors often start with tests that dont require a scope:
- Urea breath test patients drink a labeled urea solution; if H.pylori is present, the labeled carbon is released and detected in the breath.
- Stool antigen test looks for H.pylori proteins in a stool sample; its cheap and quite accurate.
- Blood antibody test useful for past infection but less reliable for active disease.
Imaging options
Can an Xray detect a stomach ulcer? The short answer is no, at least not reliably. An upper GI barium Xray can show large ulcers or complications, but many small lesions are missed. A CT scan is reserved for suspected perforation or severe bleeding.
Goldstandard: Upper gastrointestinal endoscopy
When the stakes are high, the prepyloric stomach endoscopy is the goto. A thin, flexible tube with a camera slides down the throat, giving the doctor a direct view of the ulcer and allowing a tissue biopsy. This not only confirms the ulcer but also checks for H.pylori and rules out cancer.
Endoscopy is safe serious complications occur in less than 1% of cases and most patients are out of the procedure within an hour.
Test comparison
| Test | Sensitivity | Specificity | Invasiveness | Cost (US$) |
|---|---|---|---|---|
| Urea breath test | 95% | 95% | Noninvasive | $150 |
| Stool antigen | 90% | 94% | Noninvasive | $80 |
| Blood antibody | 85% | 70% | Noninvasive | $50 |
| Upper GI Xray | 3040% | 80% | Noninvasive | $200 |
| Endoscopy with biopsy | 98% | 99% | Invasive | $1,200 |
Interpreting the results
Positive H.pylori targeted eradication
If the breath or stool test shows H.pylori, the standard regimen is a triple therapy: a protonpump inhibitor (PPI) plus two antibiotics (usually clarithromycin and amoxicillin). Recent studies note rising clarithromycin resistance, so your doctor might adjust the combo based on local data.
Negative H.pylori but ulcer present NSAIDrelated management
When H.pylori isnt the culprit, the focus shifts to stopping the irritant. Discontinuing or switching NSAIDs, adding a PPI, and protecting the stomach lining with a cytoprotective agent (like sucralfate) are typical steps.
Biopsy findings surveillance recommendations
If the biopsy shows intestinal metaplasia or dysplasia, your gastroenterologist may schedule repeat endoscopies every 612months to monitor for progression.
Treatment pathways
Medical therapy
PPIs (omeprazole, esomeprazole) are the backbone of ulcer healing. Most patients see symptom relief within a few days and complete healing in 48weeks. H2 blockers (ranitidine, famotidine) are alternatives but less potent for severe ulcers.
Lifestyle modifications
While medication does the heavy lifting, habits matter too:
- Limit alcohol and caffeine they can increase acid secretion.
- Quit smoking nicotine impairs mucosal healing.
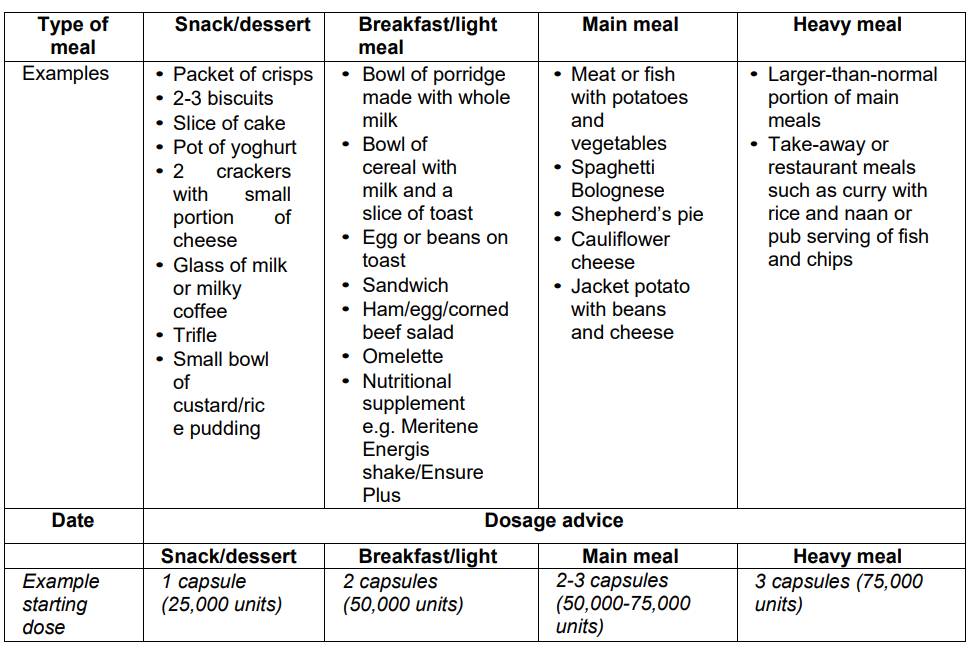
- Eat smaller, balanced meals avoid emptystomach periods that increase acid exposure.
- Manage stress through gentle exercise or mindfulness; stress alone isnt a cause, but it can magnify symptoms.
When is surgery needed?
Rarely, an ulcer will perforate, bleed uncontrollably, or cause a persistent blockage. In those cases, a surgeon may perform a laparoscopic repair or, in extreme scenarios, a partial gastrectomy.
Fastest way to cure a stomach ulcer?
Combining a highdose PPI with a full course of H.pylori eradication therapy (if the bacteria is present) typically yields the quickest healingoften within two weeks of symptom relief and full mucosal recovery by week six.
Treatment timeline chart
| Week | What to expect |
|---|---|
| 12 | Pain noticeably less, appetite returns |
| 34 | Endoscopic healing begins; sideeffects may include mild headache from PPIs |
| 56 | Most ulcers fully healed; doctor may schedule a followup endoscopy if indicated |
| 78 | Maintenance dose of PPI or stepdown to H2 blocker as advised |
Balancing benefits & risks
Benefits of early diagnosis
Finding a prepyloric ulcer before it perforates or bleeds cuts the risk of hospitalization dramatically. Early treatment also restores quality of lifeno more skipping meals or fearing nighttime pain.
Potential risks of tests & meds
Endoscopy, while safe, can cause sore throat or, rarely, bleeding from a biopsy site. Longterm PPI use has been linked to nutrient malabsorption (especially magnesium and B12) and a slight increase in certain infections. Antibiotic therapy may cause temporary diarrhea.
Shared decisionmaking tips
Ask your doctor:
- What is the exact cause of my ulcerH.pylori, NSAIDs, or both?
- Do I need an endoscopy right now, or can we start with a breath test?
- What lifestyle changes will have the biggest impact for me?
When youre in the conversation, youll feel more confident about the plan you and your doctor create together.
Expert insights
Suggested expert quotes
Dr. Laura Martinez, a gastroenterology professor at the Cleveland Clinic, notes: Endoscopic visualization remains the definitive method for diagnosing prepyloric ulcers, especially when the clinical picture is ambiguous.
Infectiousdisease specialist Dr. Anil Patel adds: Because clarithromycin resistance is on the rise, we increasingly rely on susceptibilityguided therapy or quadruple regimens to ensure eradication.
Key references to cite
When you expand this article, consider linking to:
- The Mayo Clinics overview of peptic ulcer disease
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) statistics
- Recent ACG guidelines on H.pylori management
- Evidencebased reviews on PPI safety from the American College of Gastroenterology
Further reading & patient resources
Helpful resources include patient guides from the American Gastroenterological Association and interactive symptom checkers that can help you decide when to seek care.
Conclusion
In a nutshell, diagnosing a prepyloric ulcer boils down to three pillars: recognizing the classic pain pattern, getting the right diagnostic test (usually an endoscopy paired with a breath or stool test for H.pylori), and following a proven treatment plan that combines medication with smart lifestyle tweaks. Early, accurate diagnosis dramatically lowers the risk of serious complications and speeds up recovery.
If any of the warning signs we discussed sound familiar, dont waitschedule a chat with your primarycare doctor or a gastroenterologist today. Your stomach will thank you, and youll be back to enjoying meals without the looming dread of pain.
FAQs
What are the most common symptoms of a prepyloric ulcer?
The typical signs include a gnawing or burning pain in the upper abdomen that improves briefly after eating, then returns a few hours later, along with nausea, loss of appetite, and a feeling of fullness after only a few bites.
How is prepyloric ulcer diagnosis confirmed?
Diagnosis starts with a detailed medical history and physical exam, followed by non‑invasive tests for H. pylori (urea breath test, stool antigen). The definitive confirmation is an upper gastrointestinal endoscopy with biopsy.
When is an endoscopy necessary for a suspected ulcer?
Endoscopy is recommended if there are alarm features (vomiting blood, black stools, severe pain, weight loss), if the ulcer does not heal with initial therapy, or to rule out malignancy in a confirmed ulcer.
What treatment options are most effective for a prepyloric ulcer?
The cornerstone is a proton‑pump inhibitor (PPI) plus H. pylori eradication therapy (triple or quadruple regimen) when the bacteria is present. If NSAIDs are the cause, stopping or switching the medication and adding a PPI and cytoprotective agents are advised.
Can lifestyle changes help heal a prepyloric ulcer?
Yes. Quitting smoking, limiting alcohol and caffeine, eating smaller meals, and managing stress all support healing and reduce the risk of recurrence alongside medical therapy.