What Is McMurray
The McMurray test is a simple maneuver doctors perform while youre lying on your back. By gently rotating and bending your knee, they feel for a clunk or sharp pain that suggests the meniscusthose Cshaped cartilage cushions between thigh bone and shin bonemight be torn. For patients worried about longterm joint health, understanding tests like this can help guide conversations about treatment and osteoporosis physical therapy as part of broader musculoskeletal care.
How Does It Work?
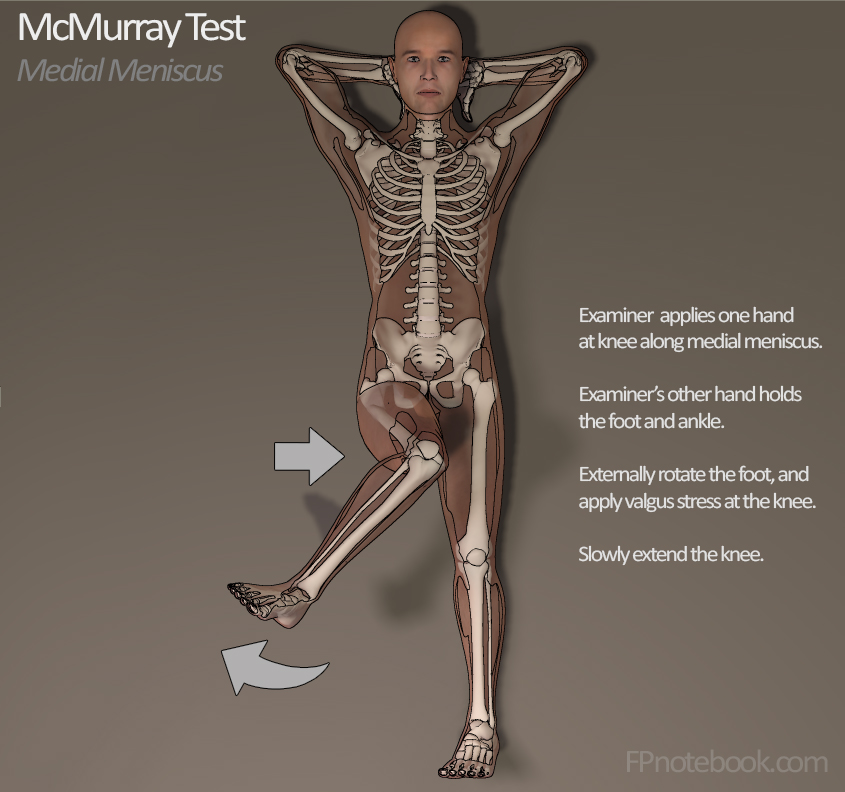
First, the examiner grasps your heel with one hand and places the other hand just above your knee joint. As they flex your knee, they rotate the tibia (shin) inward (internal rotation) and outward (external rotation) while applying a gentle valgus (pushes the knee inward) or varus (pushes outward) stress. If the meniscus is compromised, youll feel a distinct snap or hear a click.
Which Anatomy Is Tested?
The test targets the medial and lateral menisci. The medial meniscus sits on the inner side of the knee, while the lateral meniscus is on the outer side. Each one can be stressed differently, helping the examiner pinpoint where the problem lies.
Illustrative Diagram
| Step | Hand Placement | Motion |
|---|---|---|
| 1 | One hand on heel, other above knee | Flex knee to 90 |
| 2 | Apply valgus (medial) or varus (lateral) stress | Rotate tibia inward/outward |
| 3 | Extend knee slowly | Listen for click or feel for snap |
Positive Result Meaning
A positive McMurray test isnt a diagnosis on its ownits a red flag that a meniscal tear is likely. You might feel a sharp jolt, hear a click, or notice sudden knee locking. While its a reliable screening tool, clinicians usually follow up with imaging (often an MRI) to confirm the exact nature of the tear.
Is It Always a Tear?
Not always. Sometimes joint irritation, ligament laxity, or even a sloppy exam technique can mimic the findings. Thats why having an experienced practitioner and complementary tests matters.
Sensitivity & Specificity Table
| Study | Sensitivity | Specificity |
|---|---|---|
| Orthobullets Review 2022 | 78% | 87% |
| MedicalNewsToday 2023 | 71% | 84% |
| Systematic Review (PubMed) | 73% | 85% |
Medial vs. Lateral Findings
When the examiner applies a valgus stress during internal rotation, a click on the inner knee usually signals a medial meniscus issue. Conversely, a varus stress with external rotation points toward a lateral meniscus problem. Knowing the difference helps guide treatmentbecause medial tears often need different rehab protocols than lateral ones.
Medial vs Lateral
Positive Medial Meniscus
Typical symptoms: pain along the inner joint line, swelling, and a sensation of the knee giving way when you twist. The click often feels like something catching on the inside.
Positive Lateral Meniscus
Typical symptoms: pain on the outer side of the knee, occasional snapping during pivoting, and sometimes a feeling of instability, especially when standing on the affected leg.
SidebySide Comparison
| Feature | Medial Meniscus | Lateral Meniscus |
|---|---|---|
| Location of Pain | Inside joint line | Outside joint line |
| Typical Stress | Valgus + internal rotation | Varus + external rotation |
| Common Mechanism | Twisting while foot planted | Direct impact or pivot |
How To Perform
If you ever find yourself curious (or youre a sportsmedicine student), heres the McMurray test procedure broken down into bitesize steps.
Patient Positioning
Lie flat on your back with the knee relaxed. The foot should be in a neutral positionno pointing up or down.
Examiner Hand Placement
One hand holds the heel, stabilizing the foot. The other hand rests just above the knee joint, ready to feel any abnormal movement.
Movement Sequence
- Flex the knee to about 90 degrees.
- Apply a gentle valgus (push the knee inward) while internally rotating the tibia. Listen for a click.
- Return to neutral, then repeat with a varus stress and external rotation to test the lateral side.
- Slowly extend the knee while maintaining the stress; any clunk is noted.
Checklist for Clinicians
| Patient supine | Heel grip | Knee above 90 flex |
| Valgus + internal rotation | Varus + external rotation | Observe/feel for click |
For a visual walkthrough, see this .
Other Knee Tests
The McMurray test isnt the only tool in the orthopaedic toolbox. Below is a quick snapshot of how it compares to a few other common maneuvers.
Lachman Test
Focuses on the anterior cruciate ligament (ACL). The examiner pulls the tibia forward while the knee is slightly bent. A soft endpoint suggests ACL injury.
Thessaly Test
Patients stand on one leg, rotate their torso, and squat to about 20 degrees. A positive result (pain or click) also hints at a meniscal tear, and its considered quite sensitive.
Apley Test
Patient lies prone, knee flexed to 90, and the examiner pushes down (compression) or pulls up (distraction) while rotating the tibia. Compression pain points to a meniscal lesion; distraction pain suggests ligament involvement.
Comparison Table
| Test | Target Structure | Position | Sensitivity | Specificity |
|---|---|---|---|---|
| McMurray | Meniscus | Supine | 7378% | 8487% |
| Lachman | ACL | Slightly flexed | 85% | 95% |
| Thessaly | Meniscus | Standing squat | 80% | 90% |
| Apley | Meniscus/ligaments | Prone | 70% | 80% |
When To Seek Care
If youve experienced a clunk, persistent pain, swelling, or a sensation that your knee is getting stuck, its time to get professional input. Heres a quick triage:
- Redflag symptoms: Sudden inability to straighten the knee, severe swelling, or intense instability.
- Imaging options: MRI is the gold standard for visualizing meniscal tears; ultrasound can help in some cases, while plain Xrays rule out bone fractures.
- Who to see: Start with a primary care physician or sportsmedicine specialist; if the tear is complex, theyll refer you to an orthopaedic surgeon.
Treatment Options
Not every positive McMurray test ends in surgery. Treatment ranges from handsoff rest to operative repair, depending on tear size, location, and your activity goals.
Conservative Management
Most small or peripheral tears respond well to RICE (Rest, Ice, Compression, Elevation) plus a structured physiotherapy program. Physical therapists often focus on:
- Quadriceps strengthening (e.g., straightleg raises)
- Hip stabilizer work (clamshells, sidelying leg lifts)
- Proprioceptive drills (balance board, singleleg stands)
PhysicalTherapy Protocols
Core exercises might include:
- Heel slides (1015 reps, 3 sets)
- Minisquats within painfree range
- Stationary bike with low resistance for 20 minutes
Progression is guided by pain levels and swellingno rush; the meniscus heals slowly.
Surgical Options
When the tear is large, displaced, or causing mechanical locking, arthroscopic surgery is often recommended. Options include:
- Arthroscopic meniscectomy: Removal of the damaged fragment.
- Meniscus repair: Suturing the tear, especially for younger patients with good blood supply.
- Meniscus transplantation: Rare, for severe loss in highly active individuals.
Pros & Cons Table
| Approach | Pros | Cons |
|---|---|---|
| Nonoperative | Low risk, no scar, quicker initial recovery | May need longer rehab, risk of persistent instability |
| Arthroscopic meniscectomy | Fast pain relief, restores motion | Potential early onset arthritis |
| Meniscus repair | Preserves cartilage, better longterm outcomes | Longer rehab (46 months) |
Balancing Risks
Understanding both the benefits and the risks is crucial. Early detection via a positive McMurray test can prevent chronic knee problems, but overdiagnosing can lead to unnecessary imaging or surgery. The key is shared decisionmakingtalk openly with your clinician about your goals, activity level, and the realistic outcomes of each treatment path.
RealWorld Stories
Case Study: The Weekend Hiker
Emma, a 32yearold avid hiker, felt a sudden pop on a rocky trail. The onsite first aid responder performed a quick McMurray test; it was positive for the medial meniscus. Emmas doctor ordered an MRI, confirming a small, peripheral tear. Instead of surgery, she pursued a sixweek physiotherapy plan focused on quad strengthening and gait training. Six months later, she was back on the trail, painfree, and grateful for the early, accurate assessment.
Expert Insight
Dr. James Patel, an orthopaedic surgeon at a leading sportsmedicine clinic, notes, A positive McMurray test is an excellent redflag tool, but it should always be paired with imaging and a thorough functional exam. When patients understand the reasoning behind each step, compliance and outcomes improve dramatically. (Source: ).
Conclusion
A positive McMurray test is more than just a clickits a clue that your meniscus might be in trouble. By recognizing the signs, knowing how the test works, and understanding your optionsfrom simple rest to targeted surgeryyou empower yourself to make informed decisions. If youve felt that unsettling clunk or are dealing with lingering knee pain, dont ignore it. Reach out to a qualified clinician, get the right imaging, and start a tailored treatment plan. Your knees have carried you through countless steps; a little attention now can keep them moving smoothly for years to come. Whats your knee story? Share your experience in the comments, and lets keep the conversation rolling.
FAQs
What does a positive McMurray test indicate?
A positive result suggests a likely meniscal tear in the knee, but further imaging (usually MRI) is needed to confirm.
How is the McMurray test performed?
The examiner bends the knee, applies valgus or varus stress, rotates the tibia, and then extends the leg while feeling for a click or snap.
Can a positive McMurray test be a false positive?
Yes—joint irritation, ligament laxity, or an improper technique can mimic the finding, so clinical correlation and imaging are important.
What are the treatment options for a confirmed meniscal tear?
Treatment ranges from conservative care (RICE, physical therapy) to arthroscopic procedures such as meniscectomy or meniscus repair, depending on tear size and activity level.
When should I seek medical attention after a knee “click”?
If you experience persistent pain, swelling, locking, or instability, see a clinician promptly for evaluation and appropriate imaging.