Imagine tiny specks of ink slowly spreading across a clean sheet of paperthat's what pigment dispersion syndrome (PDS) does inside your eye, releasing pigment from the iris and dumping it everywhere.
If you're wondering why you're seeing floaters, why eye-pressure tests are odd, or how to keep PDS from turning into pigmentary glaucoma, read onthis guide answers the most common questions in plain language, backed by ophthalmic experts.
Quick Look Summary
Here's the headline you need to remember:
- What? Pigment dispersion syndrome is a condition where pigment granules slough off the back of the iris and settle in the eye's drainage system.
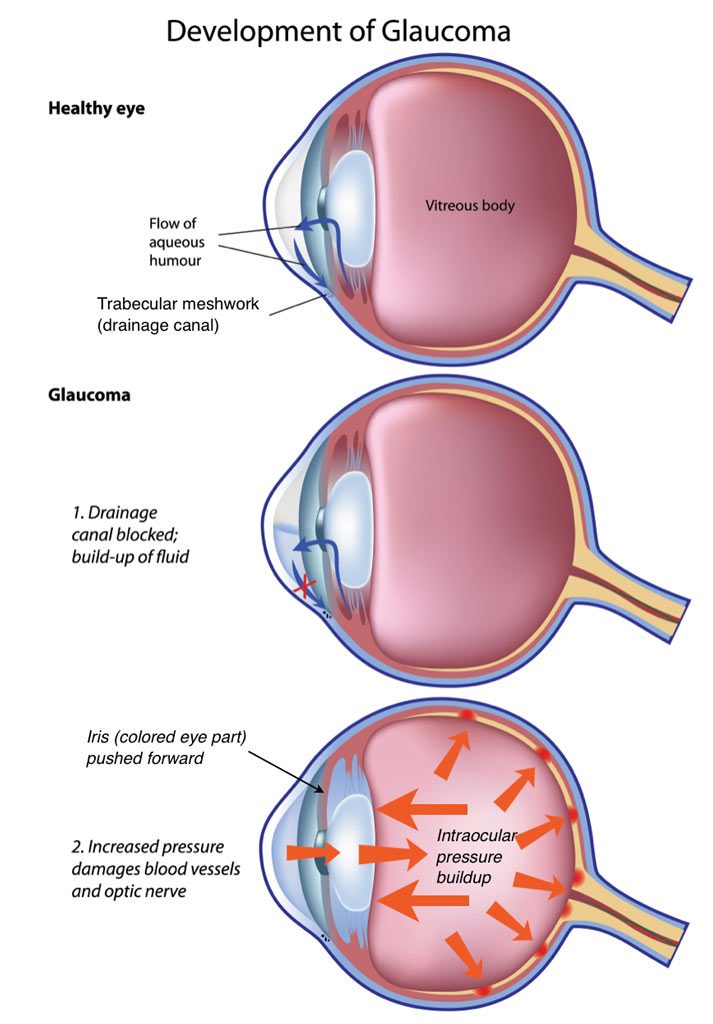
- Why care? In up to 20% of cases the pigment blocks fluid outflow, raising intraocular pressure (IOP) and potentially causing pigmentary glaucoma.
- Who gets it? Mostly young adult men (2040y) with nearsighted eyes who play high-impact sports.
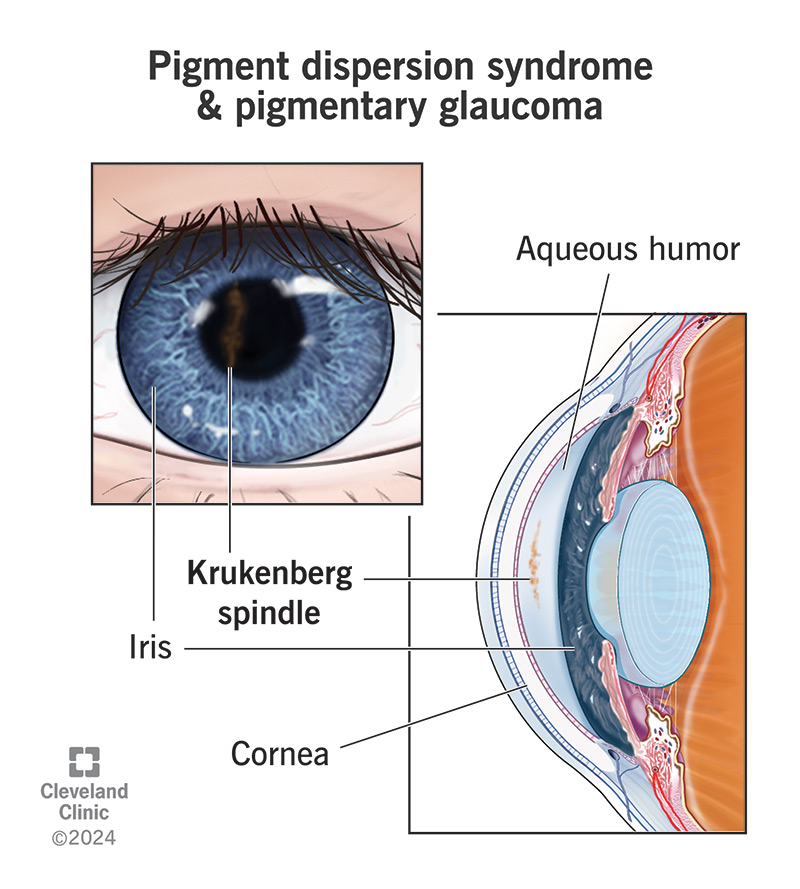
- How to catch it? Look for floaters, a Krukenberg spindle on the cornea, and pigment on the trabecular meshwork during gonioscopy.
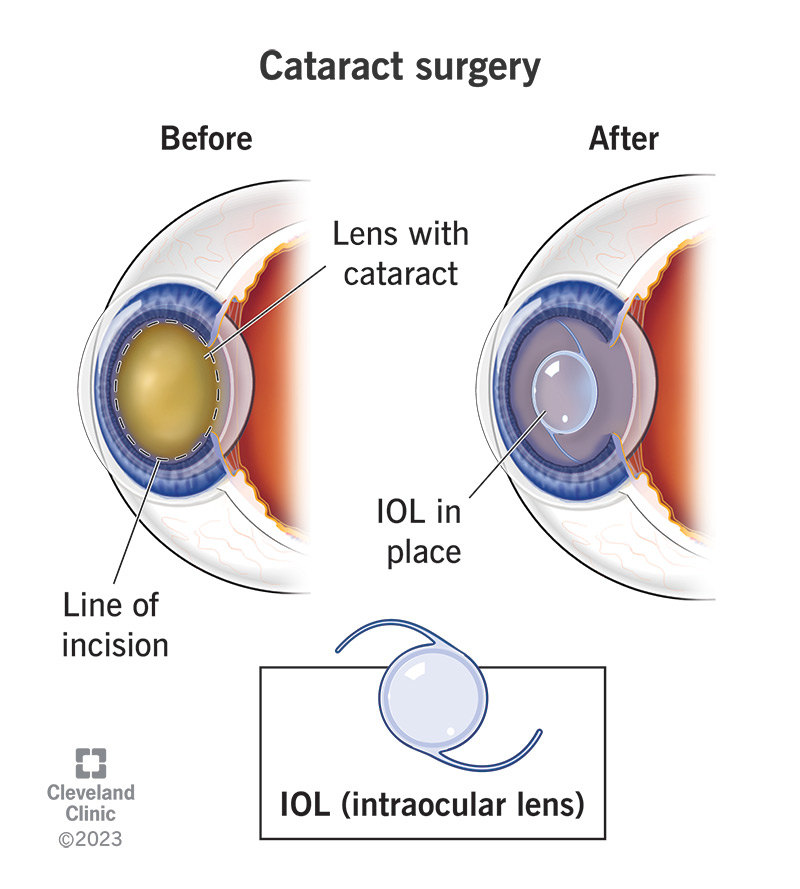
- What to do? Regular monitoring, IOP-lowering drops, laser iridotomy, or surgery if pressure spikes. If cataract surgery becomes necessary later, talk to your surgeon about post cataract glasses to optimize vision after the procedure.
Causes & Risks
Why Does the Pigment Rub Off?
The leading theory is called reverse pupillary block. When the iris bows backward during pupil dilation, it lightly scrapes against the lens zonules, shedding pigment into the anterior chamber. Over time that pigment drifts to the angle where fluid drains.
Genetics also play a roleif a close family member has PDS, you're a bit more likely to develop it. And those who love high-impact activitiesthink basketball, boxing, or mountain bikingexperience more rapid eye movements that can exacerbate the rubbing effect.
Expert Insight
According to a board-certified glaucoma specialist at the , Patients with a pronounced concave iris configuration are at the highest risk because the anatomical setup predisposes them to continuous pigment release.
Who's Most Likely?
Statistical data show a strong male predominance, especially among myopic (nearsighted) individuals. If you're a 25-year-old runner who's just started noticing strange specks floating in your vision, you fit the classic profile.
Real-World Vignette
John, a 28-year-old marathon runner, noticed tiny dust particles drifting across his field of view during long runs. An eye exam revealed a Krukenberg spindle and pigment on his trabecular meshwork. A quick gonioscopy confirmed PDS, and his ophthalmologist set up a monitoring plan that has kept his pressure stable for three years.
Signs & Symptoms
What Will You Notice?
Most people first reportthose little specks that seem to drift when you move your eyes. Others describe a raindrop shadow on the peripheral vision or a subtle haziness that comes and goes.
A clinical hallmark is the Krukenberg spindlea vertically oriented, brownish pigment line on the corneal endothelium that looks like a tiny pinwheel when you look under a slit lamp.
Comparison Chart PDS vs. Normal Aging
| Feature | Pigment Dispersion Syndrome | Normal Age-Related Changes |
|---|---|---|
| Floaters | Often numerous, appear suddenly | Gradual increase, fewer |
| Krukenberg Spindle | Present in 7080% of cases | Rare |
| Intraocular Pressure | May be elevated or fluctuate | Usually stable |
When Do Symptoms Signal Trouble?
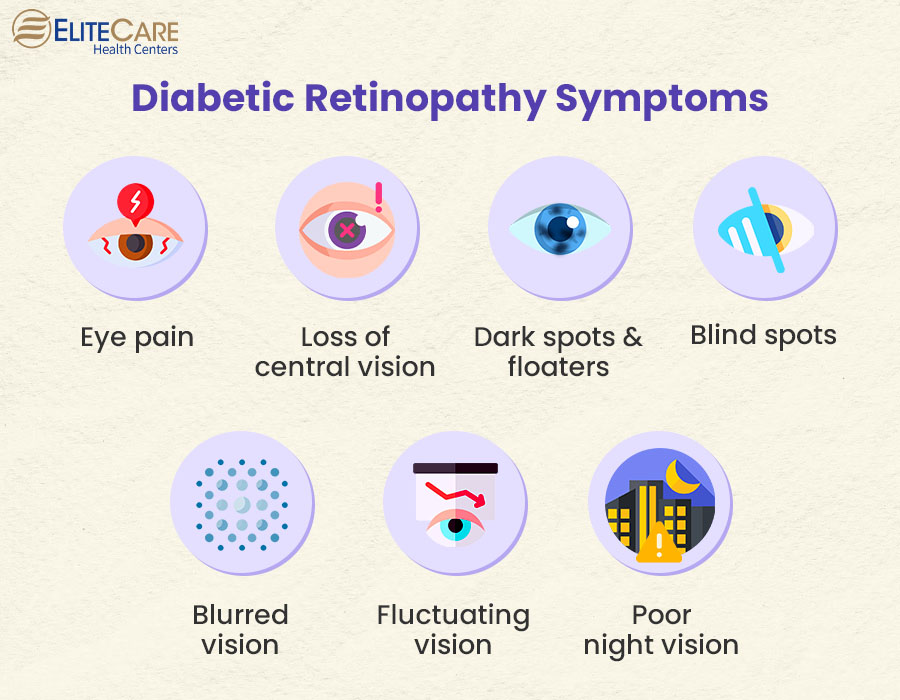
If you start feeling blurry vision, notice halos around lights, or get an eye-pressure reading above 21 mmHg, it could mean pigment has clogged the drainage angle enough to trigger pigmentary glaucoma. That's the moment you need a prompt evaluation.
Patient Checklist (Downloadable)
Feel free to copy this list onto a note-taking app:
- New or increasing floaters?
- Visible brownish line on cornea?
- Eye-pressure readings >21 mmHg?
- Any peripheral vision loss?
Diagnosis
Key Eye Exams
The diagnosis rests on three pillars:
- Slit-lamp examination reveals the Krukenberg spindle and iris transillumination defects.
- Gonioscopy the gold-standard for visualizing pigment accumulation in the angle. This is where the term pigment dispersion syndrome gonioscopy becomes relevant.
- Imaging Optical Coherence Tomography (OCT) can map the angle and quantify pigment load.
Step-by-Step Gonioscopy Guide
1. Apply a coupling gel on the prism.
2. Position the patient's head and ask them to focus on a distant target.
3. Gently tilt the prism to visualize each quadrant of the angle.
4. Look for a fine, brownish dusting on the trabecular meshworkthat's the telltale sign of PDS.
ICD-10 Coding
When your eye doctor documents the condition for insurance, they use the code H40.33 (pigment dispersion syndrome). Knowing this code can help you verify billing statements and ensure proper coverage for follow-up visits or treatments.
Reference Sources
For deeper reading, consider the and the . Both are peer-reviewed and widely cited in ophthalmology.
Treatment Options
Watchful Waiting
If your IOP is normal and your optic nerve looks healthy, many doctors recommend simply keeping an eye on thingsusually a check every six months. Lifestyle tweakslike wearing protective eyewear during contact sportscan reduce further pigment release.
Follow-Up Schedule
Years 12: Every 36 months.
Years 35: Every 612 months if stable.
Beyond 5 years: Annual exams unless changes occur.
Medications for Elevated IOP
When pressure starts creeping up, the first line of defense is eye drops. Common choices include:
- Prostaglandin analogues (e.g., latanoprost) potent IOP reducers.
- Beta-blockers (e.g., timolol) work well in combination therapy.
- Carbonic anhydrase inhibitors (e.g., dorzolamide) useful for patients who can't tolerate prostaglandins.
Pros & Cons Table
| Medication | Benefit | Potential Side-Effects |
|---|---|---|
| Prostaglandin analogues | Low dosing, strong pressure drop | Darkening of iris, eyelash growth |
| Beta-blockers | Fast onset, good for combination | Possible fatigue, bronchospasm in asthmatics |
| Carbonic anhydrase inhibitors | Useful for patients with allergies to other drops | Transient stinging, rare bitter taste |
Laser & Surgical Interventions
When drops aren't enough, we move to more definitive options.
- Laser peripheral iridotomy (LPI) creates a tiny hole in the peripheral iris, equalizing pressure across the front of the eye and stopping the reverse block mechanism.
- Filtering surgery (trabeculectomy) or MIGS (Minimally Invasive Glaucoma Surgery) creates a new drainage pathway for fluid, reserved for advanced pigmentary glaucoma. In some cases where combined pathology exists, discussion with your surgeon about cataract diagnosis test results and timing of any cataract surgery may be appropriate to coordinate care and visual rehabilitation.
Expert Commentary
A recent clinical guideline from the American Academy of Ophthalmology notes that laser iridotomy reduces the risk of progression to glaucoma in 6070% of eyes with moderate pigment accumulation. The procedure is quick, usually done outpatient, and has a low complication rate.
Lifestyle & Self-Care Tips
While medical care does the heavy lifting, a few everyday habits can make a difference:
- Wear UV-blocking sunglasses and protective goggles during high-impact or high-velocity sports.
- Stay hydratedadequate fluid intake supports normal intraocular fluid dynamics.
- Schedule regular eye-pressure checks, especially after a period of intense exercise.
PDS Survival Kit (Download)
Grab a printable PDF with do-and-don't bullet points, a reminder calendar for appointments, and a quick reference chart of medication options.
Resources & References
Below are the go-to sources that helped shape this article. They're all reputable, peer-reviewed, and written for both clinicians and patients.
- StatPearls Pigment Dispersion Syndrome (NCBI Bookshelf)
- American Academy of Ophthalmology Clinical Guidelines for Glaucoma
- Cleveland Clinic Management of Pigmentary Glaucoma
Conclusion
Pigment dispersion syndrome may start as a harmless nuisancetiny floaters and a faint brown line on the corneabut if left unchecked it can progress to pigmentary glaucoma, a vision-threatening condition. The good news? Early recognition, regular monitoring, and timely treatment (whether drops, laser, or surgery) keep most people's eyes healthy for decades.
So, if you've spotted any of the signs mentioned, schedule an eye exam ASAP. Keep a copy of the PDS Survival Kit handy, stay on top of your checkups, and don't hesitate to ask your ophthalmologist any questions that come to mind. Knowledge is power, and together we can keep your vision clear and vibrant.
FAQs
What is pigment dispersion syndrome?
Pigment dispersion syndrome (PDS) is an eye condition where pigment granules slough off the back of the iris and spread throughout the anterior chamber, eventually accumulating in the drainage angle.
Which people are most at risk for PDS?
It most commonly affects young adult men (20‑40 years) who are nearsighted and engage in activities that involve rapid eye movements or high‑impact sports.
What are the early signs I should watch for?
Typical early clues include new or increasing floaters, a brownish “Krukenberg spindle” on the cornea, and pigment deposits seen on gonioscopy of the angle.
How is pigment dispersion syndrome diagnosed?
Diagnosis relies on a slit‑lamp exam (to spot the Krukenberg spindle), gonioscopy (to view pigment in the drainage angle), and often imaging such as OCT to assess angle structure.
What treatment options are available if my eye pressure rises?
First‑line therapy is usually prescription eye drops (prostaglandin analogues, beta‑blockers, or carbonic anhydrase inhibitors). If pressure remains high, laser peripheral iridotomy or minimally invasive glaucoma surgery may be recommended.