Hey there! If youve just gotten an adrenal scan report and the words pheochromocytoma and adrenocortical carcinoma are swirling around, youre probably feeling a mix of curiosity and anxiety. Lets cut to the chase: this guide will walk you through exactly how radiology tells these two rare tumors apart, what the key imaging clues are, and why it matters for your treatment plan. No fluff, just clear, friendly explanations you can actually use.
Why Compare?
Both pheochromocytoma and adrenocortical carcinoma (ACC) originate in the adrenal glands, but they behave like night and day. A pheochromocytoma is often hormoneproducing, causing spikes in blood pressure, while ACC is an aggressive cancer that spreads quickly. Radiologists become the detectives who look for visual fingerprints that separate a friendly tumor from a dangerous one. Understanding these fingerprints helps doctors decide whether surgery, medication, or more extensive therapy is needed.
Clinical Red Flags that Prompt Imaging
Before any scan, doctors usually notice symptoms. Pheochromocytoma often shows up with sudden high blood pressure, palpitations, or sweatingthink panic attack but driven by excess catecholamines. ACC, on the other hand, may cause abdominal fullness, unexplained weight loss, or hormone excess like Cushings syndrome. When such signs appear, the radiology team is called in to provide the definitive visual answer.
What Radiologists Say About the Challenge
According to a recent RSNA abstract, radiologists find that both lesions can look surprisingly similar on noncontrast CT, which is why multiphasic protocols and careful analysis of enhancement patterns are essential. In other words, you cant rely on a single snapshot; you need a full movie.
CT vs MRI
Computed tomography (CT) and magnetic resonance imaging (MRI) each bring strengths to the table. CT is fast, widely available, and fantastic for measuring how a tumor washes out contrast over timea key point for the . MRI, with its superior softtissue contrast, highlights the tumors internal makeup, especially the classic lightbulb bright T2 signal of pheochromocytoma.
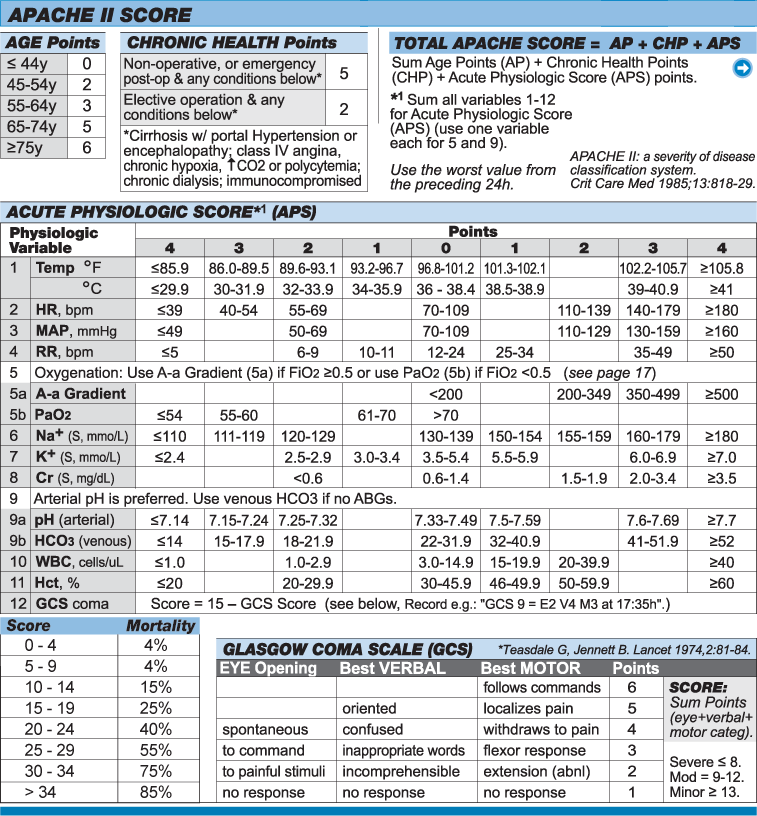
CT Protocols Youll See
Typical adrenal CT includes three phases:
- Noncontrast
- Arterial (about 60 seconds after injection)
- Venous (about 90 seconds after injection)
Radiologists then look at numbersHounsfield units (HU)to decide if a mass is likely benign, like an adrenal adenoma, or something more concerning.
CT Clues for Pheochromocytoma
Pheochromocytomas usually appear as lipidpoor lesions with a noncontrast attenuation of 3040HU. They light up brightly during the arterial phase (often >100HU) and may show a modest washout (<50%). Their size tends to be >3cm, but they rarely invade surrounding structures.
CT Clues for ACC
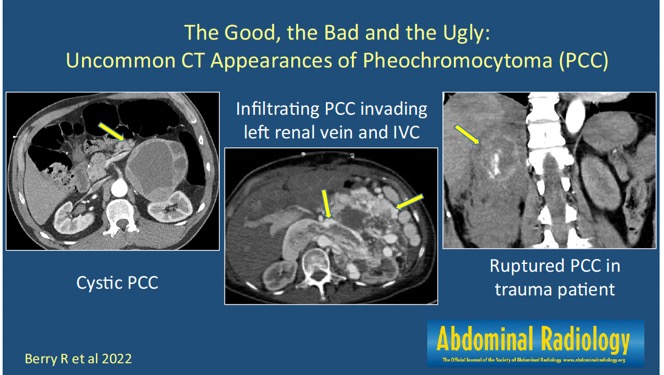
ACC lesions are typically larger (often >5cm) and heterogeneous, showing necrosis, calcifications, and a low washout (<30%). The CT may reveal capsular breach or involvement of nearby veinsred flags that point toward malignancy.
MRI Protocols That Add Confidence
MRI sequences for adrenal workup usually include:
- T1in and outofphase (helps detect intracellular fat)
- T2weighted (high signal can hint at pheochromocytoma)
- Diffusionweighted imaging (DWI) for cellular density
- Dynamic gadoliniumenhanced series
MRI Hallmarks of Pheochromocytoma
On T2weighted images, pheochromocytomas glow like a lighthouseoften called the lightbulb sign. They enhance quickly after gadolinium and may lose signal on outofphase images if theres any microscopic fat.
MRI Hallmarks of ACC
ACC shows heterogeneous T2 signal, areas of hemorrhage, and pronounced diffusion restriction, indicating dense cellularity. Postcontrast images often reveal irregular, delayed enhancement patterns and can make capsular invasion obvious.
When Functional Imaging Joins the Party
If CT and MRI still leave questionsespecially regarding metastasisdoctors may order functional studies like ^123IMIBG scintigraphy (for pheochromocytoma) or FDGPET/CT (for ACC and adrenal metastasis). These tests illuminate metabolically active tissue, helping to map spread beyond the adrenal gland.
Feature Comparison
| Feature | Pheochromocytoma | Adrenocortical Carcinoma | Typical Mimics |
|---|---|---|---|
| Size | Often >3cm, can be smaller | Usually >5cm, rapid growth | Adenoma, Myelolipoma |
| CT Attenuation (noncontrast) | 3040HU (lipidpoor) | >30HU, heterogeneous | 10HU (adenoma) |
| Arterial Enhancement | Bright, >100HU | Moderate, necrotic cores | Variable, often lower |
| Washout (venous phase) | Variable, <50% | Low, <30% | High, >60% (adenoma) |
| MRI T2 Signal | Very high (lightbulb) | Moderatehigh, heterogeneous | Fatty signal (myelolipoma) |
| Capsular Invasion | Rare | Common | Usually absent |
| Metastatic Pattern | Rare, mostly lymph nodes | Early distant mets (lung, liver, bone) | Depends on primary |
Each row in this table can be traced back to peerreviewed studieslike the AJR articles on adrenal imaging and the Radiology Assistants lesioncharacterization guideso you know the data isnt just anecdotal.
Staging & Reporting
ACC Staging on Imaging
When ACC is suspected, radiologists stage it using the ENSAT (European Network for the Study of Adrenal Tumors) system. The criteria consider tumor size, local invasion, lymph node involvement, and distant metastasis. Knowing the stage guides everything from surgical planning to eligibility for adjuvant chemotherapy.
Pheochromocytoma Reporting Checklist
A concise report for pheochromocytoma typically includes:
- Location (right vs left adrenal, extraadrenal)
- Exact size in three dimensions
- Enhancement pattern (arterial peak, washout percentage)
- Presence of necrosis or hemorrhage
- Any evidence of local invasion or distant nodules
Using the Adrenal Washout Calculator
The washout calculator is a quick spreadsheet that takes the noncontrast, arterial, and venous HU values and spits out the percentage washout. If the result is >60%, most radiologists feel comfortable labeling the lesion as a benign adenoma. Below that threshold, the lesion warrants closer scrutiny.
When to Recommend FollowUp Imaging
After surgical removal of a pheochromocytoma, most centers schedule a CT or MRI at 6month intervals for the first two years, then annually. ACC, given its high recurrence rate, often requires more intensive surveillancetypically every 34 months for the first year, then every 6 months for the next two years.
RealWorld Cases & Pitfalls
Case 1 The Sweaty Surprise
Maria, 45, presented with episodic headaches and palpitations. A 4.2cm right adrenal mass showed 38HU on noncontrast CT, surged to 115HU on arterial phase, and washed out to 28% on venous phase. MRI revealed a lightbulb bright T2 signal. Biopsy confirmed pheochromocytoma. The lesson? When you see a bright T2 signal together with low washout, pheochromocytoma becomes the top suspect.
Case 2 The Big Bad Tumor
John, 62, complained of vague abdominal fullness. Imaging uncovered a 9cm left adrenal mass with heterogeneous density, necrotic pockets, and a venousphase washout of 15%. MRI showed irregular capsular enhancement and diffusion restriction. Pathology later identified ACC. Here, size >5cm, capsular breach, and very low washout tipped the scales toward malignancy.
Common Pitfall LipidPoor Adenoma Masquerading as Malignancy
Lipidpoor adenomas can have attenuation >10HU, making them look suspicious. However, they usually demonstrate rapid washout (>60%). Using the adrenal washout calculator can prevent unnecessary alarm and invasive procedures.
BottomLine Takeaways
In a nutshell:
- Pheochromocytoma lights up on T2, shows bright arterial enhancement, and often has a modest washout.
- ACC tends to be larger, heterogeneous, invades surrounding structures, and washes out poorly.
- Combining CT and MRI gives the most reliable diagnosisdont rely on a single number.
- The is a handy safety net for differentiating benign adenomas from worrisome lesions.
- Always correlate imaging findings with clinical labs (catecholamines, cortisol) for a definitive answer.
Conclusion
Distinguishing pheochromocytoma from adrenocortical carcinoma on imaging isnt just an academic exerciseit directly impacts the treatment path, the need for surgery, and the emotional journey of patients and families. By remembering the key imaging fingerprintsbright T2, washout percentages, size thresholds, and capsular invasionyoull feel more confident interpreting reports or discussing them with your doctor. If you found this guide useful, feel free to share it with anyone navigating an adrenal mystery, and remember: youre never alone in decoding those scans.
For patients worried about recovery after adrenal surgery, consider reading about post op recovery to set realistic expectations and plan follow-up care.