If youve ever pressed a swollen ankle and felt no depression, youre looking at nonpitting edema. That firm, doughy feeling isnt just a cosmetic issue; its your bodys way of waving a red flag about something deeper.
In the next few minutes Ill walk you through the most common culprits, show you how doctors sort them out, and give you practical tips you can discuss with your clinician. Think of it as a coffeechat where we untangle the mystery together.
Quick Overview
What is nonpitting edema? Its swelling that stays firm when you press on it no dent, no pits. The fluid is rich in protein and often stuck in the tissue because the lymphatic system or other pathways cant clear it properly.
Why does it matter? While a little puffiness can be harmless, persistent nonpitting edema can signal conditions that need treatment from thyroid problems to blocked lymph vessels. Knowing the difference between pitting vs non pitting edema causes can save you time, worry, and a trip to the emergency room.
Core Causes
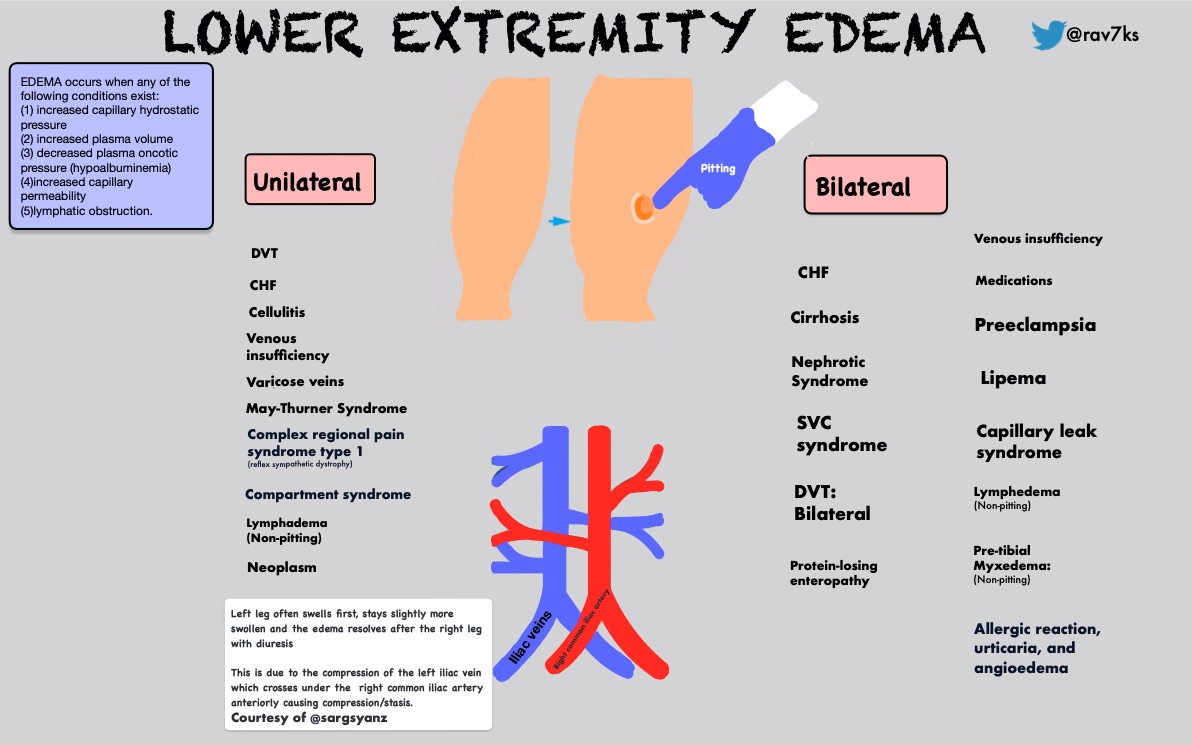
| Condition | Typical Location | Key Signs | Why It Becomes NonPitting |
|---|---|---|---|
| Lymphedema | Legs, arms | Firm, brawny skin; onesided swelling | Obstructed lymphatics trap proteinladen fluid |
| Myxedema (hypothyroidism) | Face, hands, pretibial area | Dry, thickened skin; cold intolerance | Low thyroid mucopolysaccharide buildup |
| Angioedema | Lips, eyelids, extremities (acute) | Rapid, painful swelling; no pits | Bradykinin surge increases vessel permeability |
| Lipedema | Thighs, buttocks, hips | Symmetrical fatty swelling; pain on pressure | Abnormal fat deposits overload lymphatics |
Lymphedema The Quiet Accumulator
Imagine a highway thats suddenly blocked traffic (lymph) builds up and spills over onto the shoulders of the road (your tissue). Primary lymphedema is often congenital, while secondary forms pop up after cancer surgery, radiation, or infections.
Doctors use the to grade it from Stage0 (no visible swelling) to StageIII (severe, skin changes). The grading helps decide whether you need compression garments, manual lymphatic drainage, or more intensive therapy.
Realworld glimpse
Maria, 48, noticed a tight feeling in her right ankle after a knee replacement. Pressing for a few seconds left no imprint a classic nonpitting sign. A lymphoscintigraphy confirmed lymphedema, and with a tailored compression kit, her swelling receded enough to walk her dog again.
Myxedema When Thyroid Takes a Vacation
Hypothyroidism slows everything down, including the clearance of glycosaminoglycans those sticky molecules that make skin feel waxy. The result? A pretibial myxedema that feels like a firm pillow against the shin.
Simple blood work (TSH and free T4) can nail the diagnosis. Once thyroid hormone replacement starts, youll often see the swelling soften within weeks, though the skin texture may linger a bit longer.
Quick selfcheck
Press gently on the shin for five seconds. No dent? Jot it down and ask your doctor about a thyroid panel. Early detection means you wont have to live with that stubborn puffy feeling.
Angioedema The FastActing Visitor
Angioedema shows up like a surprise party you didnt want. Within minutes, lips or eyelids puff up, and the swelling refuses to leave a pit. Triggers range from ACE inhibitors to hereditary C1esterase deficiency.
When the airway is threatened, call emergency services immediately. Otherwise, stopping the offending drug and using antihistamines or a C1esterase inhibitor can bring relief.
Fastaction checklist
- Stop any new medication (especially ACE inhibitors).
- Take an antihistamine if you have one on hand.
- If breathing feels tight, dial 911 time matters.
Lipedema The FatGirl Mystery
Lipedema mostly affects women and sneaks up during hormonal changes. The legs look heavy, but the feet stay slim a clue that the swelling isnt from fluid alone.
Unlike obesity, lipedema pain worsens with pressure and improves partially with compression. Specialized physiotherapy and, in advanced cases, tumescent liposuction can restore mobility.
Lifestyle snapshot
Wearing graduated compression stockings, staying active with lowimpact walking, and keeping a balanced diet can keep the swelling under control while you wait for a specialists assessment.
Rare Causes
Beyond the big four, a handful of conditions can masquerade as nonpitting edema:
- Filarial disease chronic parasite infection that blocks lymph vessels (common in tropical regions).
- Sjgrens syndrome an autoimmune disorder that may impair lymphatic drainage.
- Systemic amyloidosis protein deposits that harden tissues, creating a firm swelling.
- Medicationinduced calcium channel blockers or NSAIDs sometimes lead to fluid retention without pits.
When a patient mentions recent travel to an endemic area, dry eyes, or a family history of autoimmune disease, these rare culprits climb up the differential diagnosis list.
Spotting the Uncommon
History is your detectives magnifying glass. Ask about:
- Travel to subSaharan Africa or Southeast Asia (think filariasis).
- Dry mouth or eyes for months (a hint toward Sjgrens).
- Unexplained weight loss or night sweats (possible amyloidosis).
- New prescription meds, especially blood pressure drugs.
Diagnostic pearls
After a thorough exam, the next steps often involve:
- Comprehensive blood panel (CBC, CMP, thyroid, ANA, serum protein electrophoresis).
- Duplex ultrasound to rule out venous reflux.
- Lymphoscintigraphy for definitive lymphatic mapping.
- In selected cases, MRI or CT to visualize deep tissue involvement.
Diagnostic Workup
Understanding non pitting edema pathophysiology guides the tests youll undergo. Heres a simple flow you might see on the doctors office wall:
- Physical exam inspection, palpation, and the Stemmers sign (inability to pinch a skin fold on the toe).
- Lab work thyroid panel, albumin, inflammatory markers.
- Imaging duplex ultrasound first, then lymphoscintigraphy if lymphedema is suspected.
Decisiontree graphic (suggested)
Start with Is the swelling pitting? If yes, follow the pitting pathway (usually venous or cardiac); if no, dive into the nonpitting algorithm that leads you through the table of causes above.
Expert tip
According to a study published in Journal of Vascular Medicine, a simple onelayer compression test can differentiate lymphedema from myxedema: if the swelling eases under mild pressure, lymphedema is more likely.
Treatment Strategies
| Cause | FirstLine Therapy | Adjuncts | When to Refer |
|---|---|---|---|
| Lymphedema | Manual lymphatic drainage + compression garments | Lowstretch bandaging, gentle exercise | StageIIIII, recurrent cellulitis |
| Myxedema | Levothyroxine replacement | Skin moisturizers, iodinerich diet | Severe pretibial involvement |
| Angioedema | Discontinue trigger, antihistamines | Shortterm steroids, epinephrine if airway at risk | Recurrent episodes, unknown trigger |
| Lipedema | Highcompression therapy + physiotherapy | Liposuction (tumescent), dietary counseling | Painful, progressive disease |
Every treatment plan starts with the underlying cause. Thats why a precise non pitting edema differential diagnosis matters you wouldnt treat thyroid disease with compression stockings alone.
Lifestyle & SelfManagement
- Elevate the affected limb whenever possible.
- Gentle walking or swimming promotes lymph flow without stressing joints.
- Keep skin clean and moisturized to prevent cracks and infections.
- Maintain a symptom diary (photos, dates, triggers) to share with your provider.
Patient checklist for appointments
- Bring clear photos of the swelling (good for tracking changes).
- List all medications, supplements, and recent travel.
- Note any accompanying symptoms pain, itching, shortness of breath.
- Prepare questions: What tests do you recommend? How will we monitor progress?
Building Trust
All the information above is backed by reputable sources such as the and peerreviewed journals. If you ever feel uncertain, dont hesitate to ask your clinician for the studies that support their recommendations.
Remember, this guide is for education only it doesnt replace a personal medical evaluation. If swelling appears suddenly, is painful, or interferes with breathing, seek professional care right away.
Conclusion
Nonpitting edema may feel mysterious, but its usually a clue that something deeper like lymphedema, thyroid imbalance, or an allergic reaction is at play. By recognizing the hallmark signs, following a focused diagnostic workup, and matching treatment to the root cause, you can ease the swelling and restore confidence in your body.
Whats your experience with nonpitting edema? Have you found a particular therapy that helped? Feel free to share your story or ask questions were all in this together, learning and supporting each other every step of the way.
FAQs
What conditions cause non-pitting edema?
Non-pitting edema is commonly caused by lymphedema (lymphatic blockage), myxedema (hypothyroidism-related), angioedema, and lipedema (abnormal fat deposits). Other rare causes include filarial disease, Sjögren's syndrome, and systemic amyloidosis.
How can doctors differentiate non-pitting edema from pitting edema?
Doctors press the swollen area; if no indentation remains, it is non-pitting edema. Further diagnosis includes physical exam, blood tests (e.g., thyroid panel), and imaging like duplex ultrasound or lymphoscintigraphy to identify underlying causes.
What is the significance of the Stemmers sign in non-pitting edema?
The Stemmers sign is the inability to pinch a fold of skin on the toe, which suggests lymphedema, a common cause of non-pitting edema.
How is myxedema-related non-pitting edema treated?
Treatment involves thyroid hormone replacement therapy (levothyroxine), which often softens swelling over weeks, along with skin moisturizers and an iodine-rich diet in some cases.
When should a patient with non-pitting edema see a specialist?
Referral is advised for advanced stages (e.g., stage II or III lymphedema), recurrent infections, severe pretibial myxedema, unexplained angioedema episodes, or progressive lipedema symptoms requiring specialized therapy.